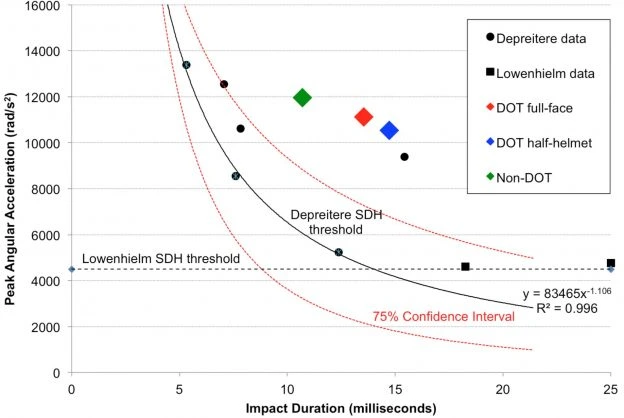
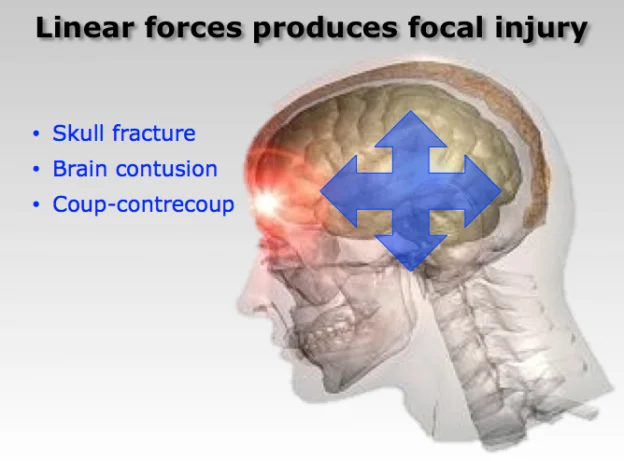
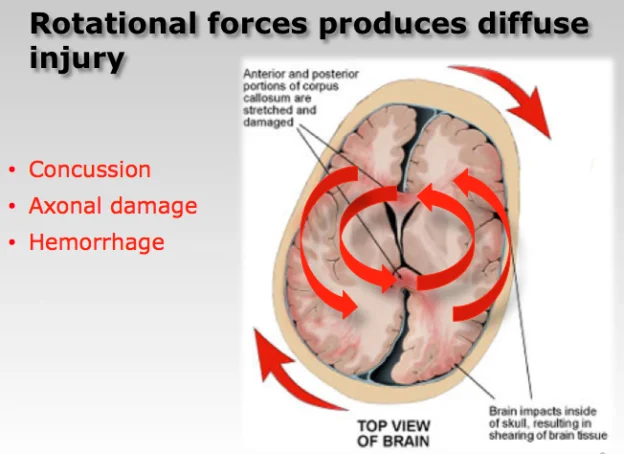
Helmets are intended to minimize blunt force trauma to the head, such as skull fracture, lacerations and contusions. Whereas risk of diffuse brain injuries, such as concussion, brain bleeding and axonal injuries are caused when brain tissue, nerves and blood vessels stretch and tear as the head moves suddenly but the brain lags behind. The type of brain injury is dependent on the magnitude of this strain and the time duration over which it acts on the brain.
Risk of focal head and brain injury is measured in terms of peak linear acceleration associated with impact, while risk of diffuse brain injury is measurable in terms of peak angular acceleration.
While helmets can prevent fatalities associated with penetrating head trauma, it may be argued that protection against diffuse brain injury is of paramount importance. After all, cuts, bruises and even bone fractures will heal, but brain injuries often have life long neurologically devastating effects.
Unfortunately, helmet testing standards addresses only the risk of blunt force trauma, not risk of brain injury.
Helmets may reduce the rotational forces acting on the brain. But since helmets are not currently certified according to their ability to protect against brain injury the level of protection is not standardized. Hence, it is possible to sustain catastrophic diffuse brain injuries, even while wearing a helmet.
As a biomechanics researcher, Dr. John Lloyd has dedicated his career to understanding the biomechanics of brain injuries. One objective of which is to develop a new generation of helmets for sports and motorcycling using “intelligent” materials that hold great promise for reducing the risk of traumatic brain injuries.
Dr. Lloyd’s biomechanics laboratory employs a specialized helmet testing apparatus for evaluating the risk of both head and brain injuries. This apparatus has been published in a peer-reviewer journal.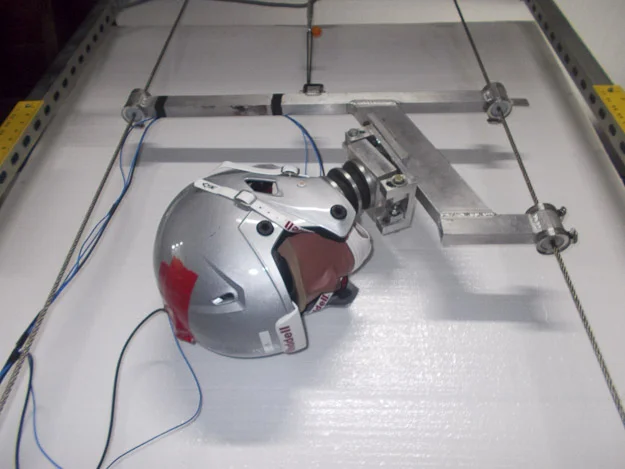 Using this apparatus, Dr. Lloyd, evaluates the linear and rotational forces associated with specific impact events, such as a motorcycle crash or sports injury, to determine whether an unhelmeted condition, or the type of helmet might have prevented the injury sustained. This apparatus has also been used to investigate whether a particular helmet failed to perform or did not meet scientifically-acceptable levels of protection.
Using this apparatus, Dr. Lloyd, evaluates the linear and rotational forces associated with specific impact events, such as a motorcycle crash or sports injury, to determine whether an unhelmeted condition, or the type of helmet might have prevented the injury sustained. This apparatus has also been used to investigate whether a particular helmet failed to perform or did not meet scientifically-acceptable levels of protection.
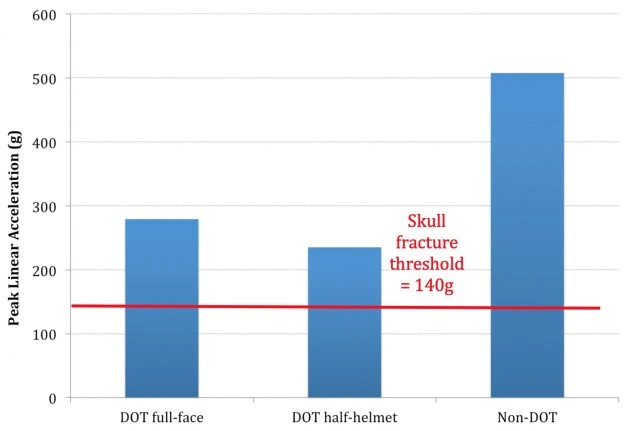
Traditional testing of motorcycle helmets focuses on reducing the effect of linear impact forces by dropping them from a given height onto an anvil and measuring the resultant peak linear acceleration. According to the Federal Motor Vehicle Safety Standard (FMVSS) 218, commonly known as the DOT helmet standard, the test involves dropping a motorcycle helmet onto a flat steel and hemispherical anvil at an impact velocity of 6.0 m/s (13.4 mph). In general, if the resultant peak linear acceleration is less than 400G, the helmet is considered acceptable. Current motorcycle helmet testing standards do not incorporate measures of angular acceleration and therefore do not address whether any motorcycle helmet can provide protection against diffuse brain injuries, including concussion.
In 1995, the European Commission Directorate General for Energy and Transport initiated a Cooperative Scientific and Technical Research (COST) program to investigate Motorcycle Safety Helmets. Several agencies from Finland, the United Kingdom, France and Germany participated in this study, which compiled and analyzed data from 4,700 motorcycle fatalities in Europe, each year. The COST report [i] documents that 75% of all fatal motorcycle accidents involve head injury. Linear forces were present in only 31% of fatal head injuries, while rotational forces were found to be the primary cause in over 60% of cases.
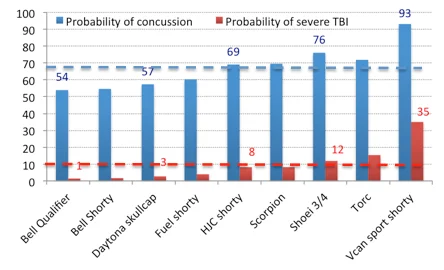
Dr. Lloyd recently conducted independent testing of various motorcycle helmets utilizing a methodology that has been peer-reviewed [i] and has survived a Daubert motion for exclusion [ii]. The following figure presents peak angular acceleration results of repeated testing of various motorcycle helmets, including: (i) Voss novelty helmet, (ii) Bell shorty helmet, (iii) Daytona shorty helmet, and (iv) Bell full-face helmet, compared with an unhelmeted condition for impacts onto concrete at approximately 20mph. The red horizontal line on the figure indicates the 50% threshold for concussive trauma, as defined by Pellman et al [iii].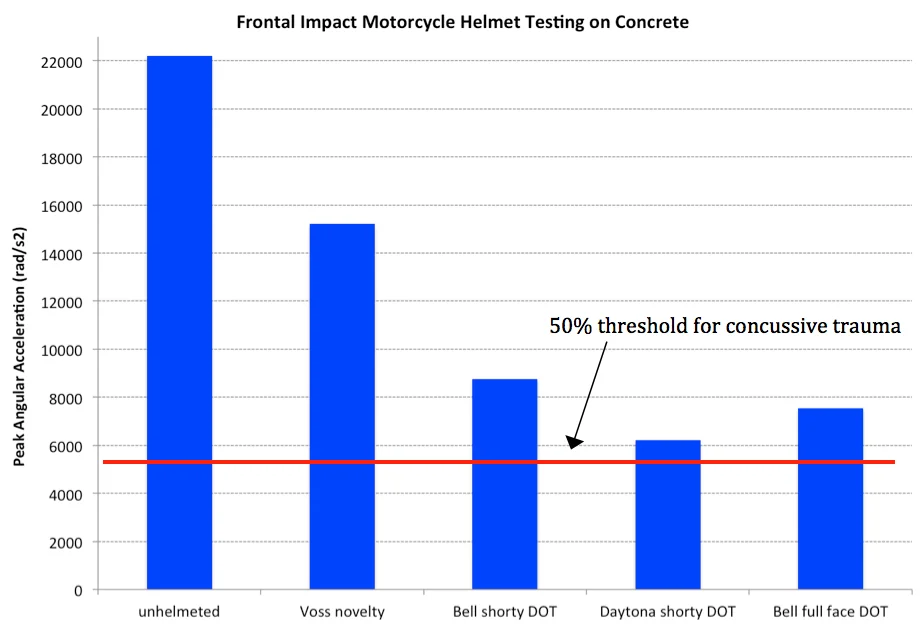
Results show that while a novelty or DOT approved motorcycle helmet will reduce the peak angular acceleration associated with a head impact relative to an unhelmeted condition, the level of protection is not sufficient to prevent diffuse brain injury in a typical motorcycle accident.
[i] Caccese V, Ferguson J, Lloyd J, Edgecomb M, Seidi M and Hajiaghamemar M: Response of an Impact Test Apparatus for Fall Protective Headgear Testing Using a Hybrid-III Head/Neck Assembly. Experimental Techniques, 2014.
[ii] Superior Court, Judicial District of Hartford, CT. Docket Number: HHD-CV-13-6043998-S. Case Caption: SHUMBO, JAKE Et Al v. K2 SPORTS USA Et Al. Order #227.86 regarding: 03/02/2015 Motion to Exclude Expert Testimony. Notice Issued: 07/09/2015
[iii] Pellman EJ, Viano DC, Tucker AM, Casson IR, Waeckerle JF: Concussion in professional football: reconstruction of game impacts and injuries. Neurosurgery 53(4): 799-812, 2003
[iv] COST-327 report of the European Commission Directorate General for Energy and Transport on Motorcycle Safety Helmets. (1999).