In a word. No.
A better question might be “Can Helmets Prevent Brain Injury?” Same answer – No.
It is not currently possible to develop a helmet that can protect all persons under all foreseen and unforeseen circumstances. But, given current medical understanding of head and brain injuries as well as 21st Century advanced materials, it is certainly possible to protect most people from life-threattening brain injuries under foreseen circumstances.
Helmets are actually intended to protect against blunt trauma injuries to the head. They are not specifically designed to prevent brain injuries.
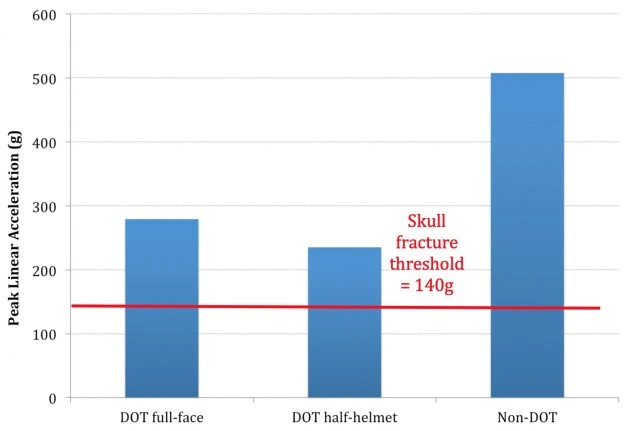
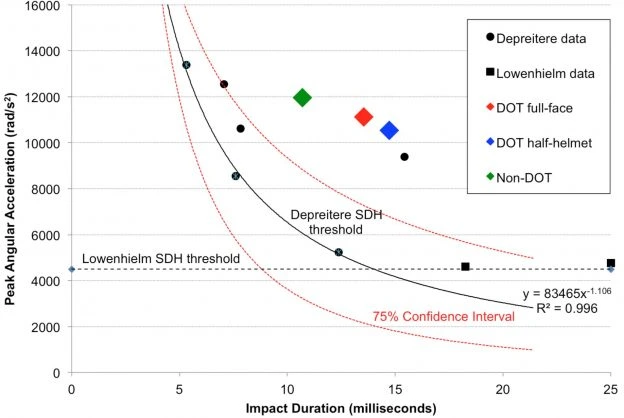
The mechanisms which cause head and brain injuries are quite different. Forces associated with linear accelerations are responsible for visible injuries, such as lacerations, contusions and skull fracture. Whereas, brain injuries, including concussions, axonal injury and subdural hematoma are caused by forces associated with angular / rotational accelerations. When the head impacts a surface, the skull may come to an abrupt stop, but inertia acting on the brain will cause it to continue to move This inertia strains the nerves and blood vessels of the brain, causing injuries. The type of injury is dependent on the magnitude of this strain and the time duration over which it acts on the brain.
Helmets may indeed reduce the rotational forces acting on the brain. But since helmets are not currently certified according to their ability to protect against brain injury the level of protection is not standardized. Hence, it is possible to sustain catastrophic brain injuries, even while wearing a helmet.
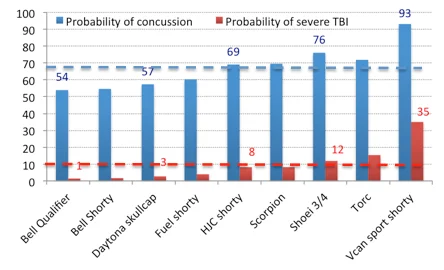
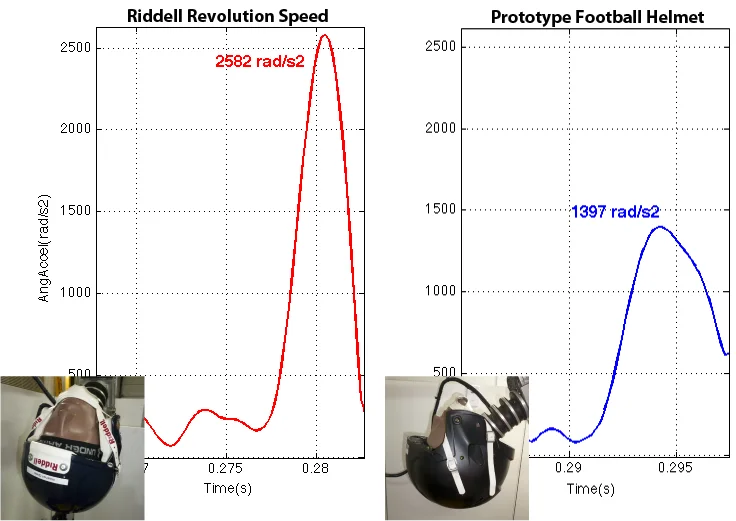
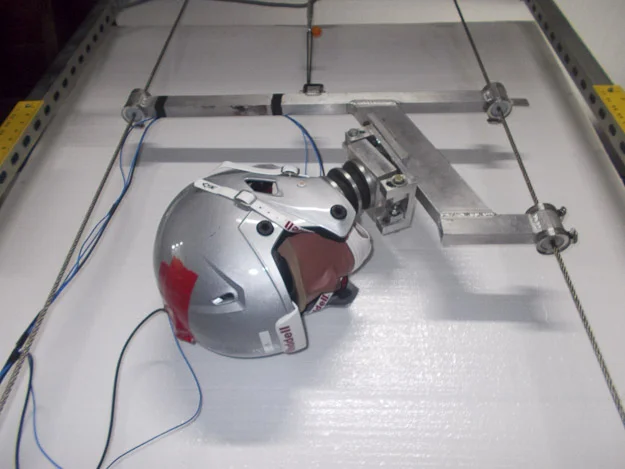
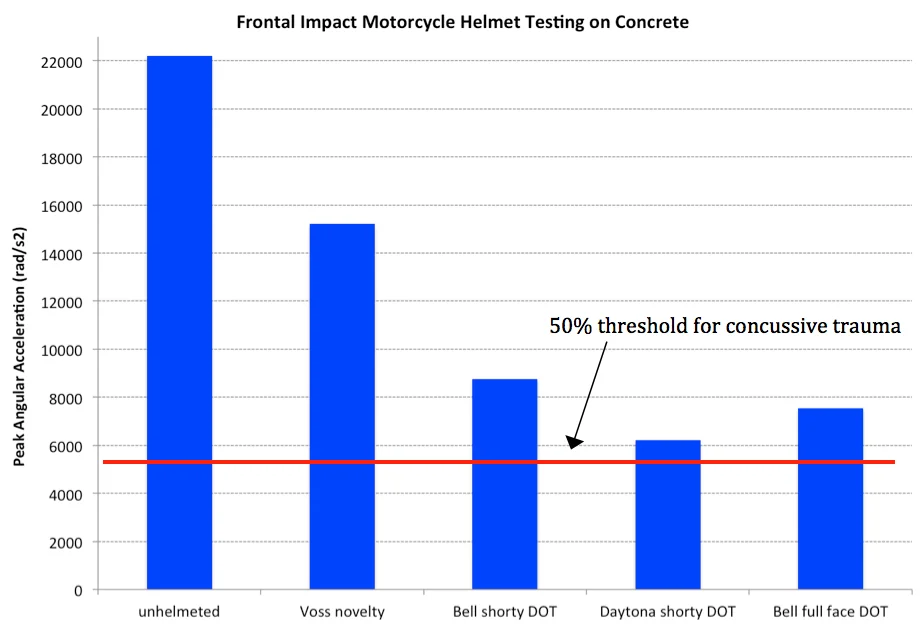
I have performed extensive biomechanical testing of helmets for various applications, including military, motorcycle, football, skiing / snowboarding and cycling. My testing involves measurement of both linear and angular accelerations, thereby characterizing helmets in terms of their ability to protect against head and brain injuries. Results vary substantially between manufacturers that offer helmets for particular applications and between applications. Based on my testing to date, I can report that certain football helmets seem to outperform helmets in other categories in terms of their ability to protect against head and brain injuries.
Much research has been conducted to understand and quantify biomechanical thresholds for various head and brain injuries, including skull fractures, concussions, axonal injury (damage to nerve fibers in the brain) and subdural hematomas (bleeding in the brain). Why then don’t all helmet manufacturers strive to provide necessary protection?
There are certain intrinsic or personal factors that might increase one’s risk of head and brain injury, but for the rest of us, why do helmets provide inadequate protection against life-threatening head and brain injuries during reasonable or foreseen use?
One example of this is the life-threatening brain injury which former Formula One superstar, Michael Schumaker sustained when he fell while skiing and impacted a rock. It has been reported that Mr. Schumaker was only skiing at about 13mph when he fell and the likelihood of impacting a fixed object while skiing, such as a tree or rock is certainly not unforeseen. So why did his helmet fail to provide necessary protection?
Advanced materials certainly exist to provide required protection for normal persons, including Mr. Schumaker and many other unfortunate victims, under normal or foreseen circumstances. As end-users, we must demand that regulatory organizations require helmet manufacturers meet standards that protect persons who are not otherwise at heightened risk from head and brain injuries due to foreseen circumstances.