Helmet expert Dr. John Lloyd has served attorneys nationwide for 25+ years in biomechanics, human factors, helmet testing and motorcycle accident expert
I am a motorcycle enthusiast with 40+ years of experience in the saddle and a biomechanics researcher focusing on head and brain injury. Over the years I performed more than 2600 helmet impact tests, including 328 motorcycle helmets. The following are my take-away points for motorcyclists:
Helmets are the best protection we have against head and brain injuries. That said, standard certified motorcycle helmets are only 37-42% effective in preventing fatal head injuries.
Helmets are designed after ancient military helmets to serve as a second skull and thereby protect the head against penetrating injury.
Helmets, in general, are not intended to protect against brain injury.
There are two types of head and brain injuries, which are caused differently:
Translational (linear) forces cause focal injuries including cuts, bruises, and skull fractures.
Tangential forces cause rotational injuries including concussion, brain nerve damage, and brain bleeding.
Translational and tangential forces are generated in every impact
Certified motorcycle helmets do a great job of protecting against focal head injuries.
My research shows that DOT-certified motorcycle helmets reduce the risk and severity of focal injuries by 93 percent.
Novelty (non-certified) helmets do not offer any protection against focal injuries.
It is therefore highly recommended that riders wear a certified motorcycle helmet at all times.
Helmets that offer greater coverage, i.e. open-face (3/4) and full-face helmets, provide the best protection against focal injuries. However, the US DOT standard (FMVSS 218)[i] does not require impact testing of the chin bar, therefore there is no certified protection against facial injuries for full-face helmets that are only certified to the DOT standard.
Generally, certified motorcycle helmets do not protect against rotational brain injuries. In fact, on average, a standard certified motorcycle helmet will actually increase the rider’s risk of concussion, nerve damage (axonal injury), and brain bleeding (subdural hemorrhage) by 19 percent, compared to an unhelmeted head impact.
Rotational brain injuries are the cause of fatalities in two-thirds of all helmeted motorcycle deaths.
It has been shown that, in general, larger and heavier helmets increase the risk of rotational brain injuries, including concussion, axonal injury, and brain bleeding because they generate greater impact-related rotational forces on the brain.
So, what can a safety-minded rider do to minimize their risk?
Revised motorcycle helmet standards are starting to look at brain injury risk. The new ECE 22.06[ii] and Snell M2025[iii] standards now measure the risk of rotational brain injury, though the passing threshold is 23% risk of neurologically devastating or potentially fatal rotation brain injury, at a moderate impact speed of 17.5 mph.
My recommendation is to choose a helmet that meets either the ECE 22.06 or Snell M2025 standard, in addition to whatever standard is mandated in your country.
Choose a lighter, smaller helmet with the desired coverage over a larger, heavier helmet. Not only will this likely provide better protection against rotational brain injuries, but will also generate less wind resistance and be more comfortable on those longer rides.
Consider helmets that incorporate new technologies that are intended to reduce the risk of rotational brain injuries. Such technologies include the omni-directional protection system and the multi-directional protection system (MiPS).
Don’t buy a helmet just based on looks, make an informed purchase based on fit and protective performance.
What can motorcycle helmet manufacturer’s do to improve helmet performance?
Current motorcycle helmet designs may be over-engineered to reduce translational forces that cause focal head injuries, resulting in helmets that are larger and heavier, thereby increasing the risk of rotational brain injuries, which are the primary cause of fatality in two-thirds of helmeted motorcycle crashes. Protection against focal injuries is important, but needs to be balanced against increased risk of rotational brain injuries. Manufacturers should evaluate materials that allow the development of smaller and lighter helmets.
A meta-analysis is underway, comparing helmets intended for a variety of activities including motorcycling, skiing, bicycle, off-road, American football, ice hockey and military. Preliminary results suggest that helmets intended for other sports activities may outperform motorcycle helmets at similar impact speeds in terms of protection against both focal head injuries and rotational brain injuries
[i] U.S. Department of Transportation (2013) Federal Motor Carrier Safety Administration Standard No. 218, Motorcycle helmets. Washington, DC.
[ii] United Nations (2021). Uniform Provisions Concerning the Approval of: Protective Helmets, of their Visors and of their Accessories for Drivers and Passengers of Motorcycles and Mopeds. Regulation No. 22-06
[iii] Snell Memorial Foundation. (2024). Standard for Protective Headgear for use with Motorcycles and Other Motorized Vehicles. M2025
2002-2022 Courtesy Assistant Professor Department of Chemical and Biomedical Engineering, College of Engineering, University of South Florida, Tampa, FL
09/11-02/16 Director of Traumatic Brain Injury Laboratory / Program Specialist James A Haley Veterans Hospital, Tampa, FL
08/09-09/11 AssociateDirector Veterans Administration, Health Services Research and Development (HSR&D) / Rehabilitation Research and Development (RR&D) Research Center of Excellence, Tampa, FL
10/99-08/09 Director of Research Laboratories Patient Safety Center of Inquiry, James A. Haley Veterans Hospital, Tampa, FL
05/98-05/00 Director of Information Systems UTEK Corporation, Plant City, FL
06/96-10/99 ActingDirector Center for Product Ergonomics, University of South Florida, Tampa, FL
01/96-05/96 Ergonomics Laboratory Manager/ Research Ergonomist Center for Product Ergonomics, University of South Florida, Tampa, FL
07/93-01/96 Principal Ergonomist The Ergonomics Institute, Hauppauge, NY
07/92-07/93 Ergonomics /Biomechanics Consultant Biomechanics Corporation of America, Melville, NY
07/90-07/91 Research Ergonomist Liberty Mutual Research Center, Hopkinton, MA
12/88-07/90 Human Reliability Consultant R M Consultants Ltd., Warrington, Cheshire, England
Columnist for Ergonomics Intelligence Report, James Publishing, Santa Ana, CA
Book reviewer for Ergonomics In Design, Human Factors and Ergonomics Society
Journal of Rehabilitation Research and Development, Department of Veterans Affairs, Washington, DC
Applied Ergonomics, Taylor and Francis, London
Ergonomics, Taylor and Francis, London
Department of Veterans Affairs HSR&D Scientific Merit Review Committee
Department of Veterans Affairs RR&D Scientific Merit Review Committee
Natural Sciences and Engineering Research Council of Canada (NSERC), grant reviewer for federal funding agency
Applied Ergonomics Journal
National Neurotrauma Society 2016 Symposium
Journal of Safety
New England Journal of Medicine
Nebraska University Press
Journal of Forensic Sciences
Grants and Funded Research
‘Biomechanical assessment of dynamic postural sway in healthy elderly.’ Role: Co-Investigator. Sponsored by Institute for Aging. Awarded $7,500, 1996.
‘Redesigning patient handling tasks and equipment to prevent nursing back injuries.’ Role: Co-Investigator. Sponsored by Department of Veterans Affairs RR&D. Awarded $305,000, 1997.
‘Effect of wrist exposures on median nerve conduction: Pilot study.’ Role: Co-Investigator. VA RR&D. Awarded $50,000, 1997.
‘Evaluation prototype: Exam room of the future.’ Role: Co-Investigator. Sponsored by BHM Medical, Inc. and Department of Veterans Affairs. Awarded $60,000, 1998.
‘Patient Safety Center of Inquiry.’ Role: Associate Director and Co-Investigator. Sponsored by VA HSR&D. Awarded $1,500,000, 1999.
‘VISN-Wide Deployment of a Back Injury Prevention Program for Nurses: Safe Patient Handling and Movement.’ Role: Co-Investigator. Sponsored by VA HSR&D. Awarded $2.4 million, 2001.
Research Enhancement Award Program: ‘Safe Patient Mobility.’ Role: Associate Director and Co-Investigator. Sponsored by VA HSR&D. Awarded $1.1 million, 2001.
‘Development and Validation of Measurement System to Quantify Spinal Compression.’ Role: Co-Investigator.’ Sponsored by VISN8 Patient Safety Center of Inquiry. Awarded $5,000, 2001.
Research Enhancement Award Program: ‘Technology to Prevent Adverse Events in Rehabilitation.’ Role: Associate Director and Co-Investigator. Sponsored by VA RR&D. Awarded $1.35 million, 2002.
Enhancement of RR&D Research Laboratory Capabilities at the Tampa Veterans Administration Medical Center. Role: Principal Investigator. Sponsored by VA RR&D. Awarded $125,000, 2002.
‘Biomechanical assessment of wheelchair transfers toward upper extremity preservation in persons with SCI.’ Role: Co-Principal Investigator. VA RR&D. Awarded $50,000, 2002.
‘Patient Safety Center of Inquiry.’ Role: Associate Director and Co-Investigator. Sponsored by VA HSR&D. Awarded $2,000,000, 2003.
‘Development of an Instrumented Mannequin for Restraint and Control Training,’ Role: Principal Investigator. Sponsored by Department of Veterans Affairs, Office of Occupational Health and Safety. Awarded $75,000, 2003.
‘Validation of the Actiwatch as a Pain Treatment Outcome Measure.’ Role: Co-Investigator. Sponsored by VA RR&D. Awarded $200,325, 2005.
‘Folding Motorized Prone-Cart.’ Role: Co-Investigator. Sponsored by VA RR&D. Awarded $357,100, 2005.
‘Development of Force Gloves for Biomechanical Evaluation of Dynamic Patient Handling Tasks.’ Role: Co-Investigator. Sponsored by University of South Florida Patient Safety Foundation. Awarded $7,000, 2005.
‘Biomechanical Evaluation of Patient Transport Activities.’ Role: Co-Investigator. Sponsored by University of South Florida Interdisciplinary Grant Program, Dane Industries, Inc. Awarded $25,000, 2005.
Tampa VA Shared Equipment Evaluation Program. VHA. Awarded $272,000, 2005.
‘Evaluation of Assistive Transfer Devices to Preserve UE Function in SCI.’ Role: Principal-Investigator. Sponsored by VA RR&D. Awarded $474,300, 2007.
Center of Excellence: ‘Maximizing Rehabilitation Outcomes.’ Role: Associate Director. Sponsored by VA HSR&D / RR&D. Awarded $4,100,000, 2009.
‘Development of Headwear to Prevent Fall-Related Injuries in Elderly Persons.’ Role: Co-Investigator / Biomechanist. Sponsored by National Institutes of Health, Small Business Innovation Research. Awarded $1,000,000, July 2010.
‘Threats to Skin Integrity Associated with Ceiling Lift Sling Use in Persons with SCI.’ Role: Principal Investigator. Sponsored by Department of Veterans Affairs, Office of Occupational Health and Safety. $600,000, February 2011.
‘Biomechanical Evaluation of Techniques Associated with Prevention and Management of Disturbed Behavior – Phase 2’ VA Portland. Role: Principal Investigator. Awarded $60,000, February 2011.
Equipment grant for Traumatic Brain Injury program. VA RR&D. Role: Principal Investigator. Awarded $239,000, April 2011
‘Biomechanical Evaluation of Techniques Associated with Prevention and Management of Disturbed Behavior – Phase 3’ VA Portland. Role: Principal Investigator. Awarded $68,700, December 2011.
Development and Evaluation of a Sling-Less Lift System. VA RR&D. Role: Principal Investigator. Awarded $730,000. ** best proposal score in history of JAHVA
Development of Motorcycle Helmets to Protect Against Traumatic Brain Injury. CDC / NCIPC. Role: Principal Investigator. $225,000. Submitted April 2015. Not funded
Lloyd JD and Baptiste A, “Patient Handling Technologies.” In: Charney, W (ed.). Handbook of Modern Hospital Safety, second edition. Taylor and Francis 2009
Pappas IP, Del Rossi, G, Lloyd J, Gutmann J, Sackellares CJ et al. Synchronization and network measures in a concussion EEG paradigm. In Models, Algorithms and Technologies for Network Analysis. 2014.
Lee WA and Lloyd JD “Biomechanical, Epidemiologic and Forensic Considerations of Pediatric Head Injuries” In Freeman MD and Zeegers M (eds). Forensic Epidemiology: Principles and Practice. Elsevier publishers, Oxford UK. 2016.
Lloyd JD and Kelleher, V, (2000). Patient safety center of inquiry plans effective dissemination of its findings throughout the VA. Veterans Health System Journal Aug 55–56.
Nelson A, Owen B, Lloyd JD, Fragala G, Matz M, Amato M, Bowers J, Moss-Cureton S, Ramsey G and Lentz K, (2003) Safe Patient Handling and Movement: Preventing back injury among nurses requires careful selection of the safest equipment and techniques. American Journal of Nursing 103(3): 32–43
Barrett B, Phillips S, Lloyd J, Cowan L, Friedman Y et al. (2022) Evaluation of Protective Properties of Commercially Available Medical Helmets: Are Medical Helmets Protective? Journal of Patient Safety 18 (1).
Lloyd JD: (1995) Getting Injured Employees Back to the Workplace – Return to Work Planning. Workplace Ergonomics Magazine Steven Publishing, TX
Lloyd JD: (1995) A Holistic Ergonomic Approach for Successful Return to Work. Chartered Property Casualty Underwriters Society, Malvern, PA
Lloyd JD and Gross C: (1996) Ergonomic evaluation of pen design and writing characteristics. Ergonomics Intelligence Report James Publishing, Santa Ana, CA
Lloyd JD and Gross C: (1996) Biomedical stress test for carpal tunnel syndrome. Ergonomics Intelligence Report James Publishing, Santa Ana, CA
Lloyd JD: (1996) How to correctly set up an ergonomic office workstation. Ergonomics Intelligence Report James Publishing, Santa Ana, CA
Lloyd JD: (1996) A checklist for the evaluation of ergonomic stress at computer workstations. Ergonomics Intelligence Report, James Publishing, Santa Ana, CA
Gross C, Lloyd JD and Tabler R: Ergonomic Analysis of Pen Comfort and Wrist Dynamics While Writing. Unpublished. University of South Florida, Tampa, FL
Gross C and Lloyd JD: (1997) HumanTRAC: A New Method for Rapid Product Ergonomic Assessments. Unpublished. University of South Florida, Tampa, FL
Powell-Cope G, Moore H, Kearns W, Baptiste A, Lloyd JD, Applegarth S and Nelson A. (2005). The Case for Preventing Wandering and Associated Adverse Events for Veterans with Dementia. TIPS Nov/Dec 5(6): 3
Research Basis for the Development of a Dynamic Median Nerve Stress Test. Proceedings of American Occupational Health Conference. Orlando, FL, May 16, 1997
‘Work-related carpal tunnel syndrome’. Presented at Alabama Governor’s safety and health conference. Birmingham, AL. August 29, 2000
Lloyd JD and Westhoff O. Development of an Intelligent Mannequin for Research in Safe Patient Handling and Movement. Proceedings of the Sixth Annual Safe Patient Handling and Movement Conference. Clearwater, FL, March 2, 2006
Lloyd JD. Biomechanical Evaluation of Patient Transport Technologies – a project in development. Proceedings of the Sixth Annual Safe Patient Handling and Movement conference. Clearwater, FL, March 2, 2006
Belsole RJ and Lloyd JD. Repetitive wrist movements: an adverse effect on median nerve conduction. American Society for Surgery of the Hand (ASSH). 54th Annual Meeting, 1998.
Lloyd JD and Belsole RJ. Neurovascular considerations of median nerve neuropathy and implications for clinical diagnosis. American Society for Surgery of the Hand (ASSH). 54th Annual Meeting, 1998.
Lloyd JD and Belsole RJ. Repetitive wrist movements: an adverse effect on median nerve conduction. University of South Florida Health Sciences Center Research Day, February 1999.
Lloyd JD, Nelson AL, Gross CM and Menzel N. Redesigning Patient Handling Tasks and Equipment to Prevent Nursing Back Injuries. Department of Veterans Affairs, Health Services Research and Development. 19th annual meeting, February 2001.
Lloyd JD. Repetitive Wrist Movements: Clinical Implications for Ergonomic Workplace Surveillance. International Society for Occupational Ergonomics and Safety annual meeting, June 2005.
Lloyd JD. Clinical Biomechanics of Wheelchair Transfers and Repositioning Tasks in SCI. 20th Congress of the International Biomechanics Society and 29th Annual Meeting of the American Society of Biomechanics, August 2005.
Lloyd JD and Harrow JJ. Clinical Biomechanics of Wheelchair Transfers in Spinal Cord Injury. American Paraplegic Society Annual meeting, September 2005.
Harrow JJ and Lloyd JD. Biomechanical Assessment of Pressure-Relief and Repositioning Tasks in Persons with SCI. American Paraplegic Society annual meeting, September 2005.
Lloyd JD and Harrow JJ. Clinical Biomechanics of Wheelchair Transfers in Spinal Cord Injury. American Association of SCI Nursing annual meeting, September 2005.
Harrow JJ and Lloyd JD. Biomechanical Assessment of Pressure-Relief and Repositioning Tasks in Persons with SCI. American Association of SCI Nursing annual meeting, September 2005.
Lloyd JD and Harrow JJ. Biomechanical Assessment of Independent Wheelchair Transfers in Persons with SCI. American Association of SCI Nursing annual meeting, September 2006.
Campbell RR, Lloyd JD and Gutmann J. VHA Trends in the total costs of care for the polytrauma cohort: Disproportionate impact of post-acute inpatient care. Federal Interagency Conference on Traumatic Brain Injury, 2011
Lloyd JD, Gutmann J and Arslan O. Toward Biomechanical Understanding of Brain Kinematics Associated with TBI using cadaveric specimens. Federal Interagency Conference on Traumatic Brain Injury, 2011
Lloyd JD, Gutmann J and Del Rossi G. Do Ill-Fitting Helmets Amplify the Risk of Head Injury Among Youth Football Players? – A Biomechanical Analysis, with Discussion for Applicability to Military Protection. Federal Interagency Conference on Traumatic Brain Injury, 2011
Lloyd JD, Gutmann J, Craighead J & Del Rossi G. Do Helmets Prevent Concussion? 8th Annual Conference of Blast TBI, December 2011, Tampa.
Lloyd JD, Gutmann J, Craighead J & Arslan O. Biomechanics of Blast TBI. 8th Annual Conference of Blast TBI, December 2011, Tampa.
Lloyd JD & Lee WE. Biomechanics of Inflicted Head Trauma. Presented at 4th Penn State Hershey International Conference on Pediatric Abusive Head Trauma, June 27-28, 2013, Burlington, VT.
Sackellares JC, Lloyd J & Vega D EEG of Concussive Impact in Football. Submitted to American Academy of Sports Neurology Sports Concussion meeting, July 2014. Chicago.
Lloyd J & Conidi F. Preventing Concussion in Sports – A Proposed Biomechanical Threshold. Submitted to American Academy of Sports Neurology Sports Concussion meeting, July 2014. Chicago.
Lloyd JD. Military Helmets May Provide Little Protection Against Traumatic Brain Injury. Presented at Military Health System Research Symposium, August 2014. Fort Lauderdale.
Lloyd JD & Conidi FX. Biomechanical Evaluation of Helmet Protection Against Concussion and TBI. Presented at International State-of-the-Science Meeting on the Biomedical Basis for Mild Traumatic Brain Injury (mTBI) Environmental Sensor Threshold Values. November 2014. MacLean, VA.
Lloyd JD, Sabbagh J & Dickey C. Investigating the Effects of Mild Blast Injury on TBI Symptoms and Tau Pathology. Presented at International State-of-the-Science Meeting on the Biomedical Basis for Mild Traumatic Brain Injury (mTBI) Environmental Sensor Threshold Values. November 2014. MacLean, VA.
Conidi FX and Lloyd JD. Incidence of Traumatic Brain Injury in retired NFL Players. Correlation with Diffusion Tensor MRI Imaging and Neuropsychological Testing. Annual meeting of the American Academy of Neurology. 2016.
Lloyd J. Brain Injury in Sports. North American Brain Injury Society 13th Annual Conference on Brain Injury. 2016.
Lloyd J. Biomechanics of Motorcycle Helmet Protection. National Neurotrauma Society. 2016.
Lloyd JD: Controls and displays. In: Whalley S et al: Ergonomic guidelines for the offshore oil and gas industry. R.M. Consultants Ltd., Warrington, England, 1989.
Lloyd JD: Cumulative trauma disorders of the upper extremities – Experiment report: Liberty Mutual Insurance Co., Boston, MA, 1991.
Lloyd JD: A human factors approach to the design and implementation of mobile data terminals in British Gas service engineer’s vehicles. Thesis – University of Technology, Loughborough, Leicestershire, England, 1992.
Nair C and Lloyd JD: Ergonomic assessment of the N250 flight deck. PT. Industri Pesawat Terbang Nusantara, Indonesia, 1992.
Rome D, Ratner D, Braveman K and Lloyd JD: Mannequin tutorial. In: Mannequin High – ergonomics in design. Biomechanics Corporation of America, Melville, NY, 1992.
Lloyd JD: Ergonomic assessment of risk and liability for heavy electronics manufacturing facility. Square D Company, Smyrna, TN, 1992.
Lloyd JD: AADCAS Phase II – a comprehensive anthropometry and reach study using sonic digitization techniques. Grumman Aircraft Systems, Grumman Corporation, Bethpage, NY, 1992.
Lloyd JD: Ergonomic workplace assessment for materials handling operations. Fujitsu Network Transmission Systems Inc., Richardson, TX, 1993.
Lloyd JD: Ergonomic assessment of risk and liability for a precision electronics assembly process. Fujitsu Network Transmission Systems Inc., Richardson, TX, 1993.
Lloyd JD: Corporate ergonomics program for safety and environmental compliance. Biomechanics Corporation of America, Melville, NY, 1993.
Lloyd JD: Ergonomic assessment of risk and liability, including NIOSH lifting evaluation. Philip Morris USA, Cabarrus Manufacturing Center, NC, 1993.
Lloyd JD: Engineering Workplace Assessment. Sony Music, Carrolton, GA, 1993.
Lloyd JD: Ergonomic assessment of risk and liability for aftermarket product manufacturing division. Allied Signal, Greenville, OH, 1993.
Lloyd JD: Wrist Stress Determination. U.S. Surgical Corporation, CT, 1993.
Lloyd JD: Ergonomic assessment of risk and liability for heavy assembly operation. Nevamar Corporation, Odenton, MD, 1993.
Lloyd JD: Ergonomic assessment of risk and liability for a medical laboratory. MetPath Laboratories, PA, 1993.
Lloyd JD: Ergonomic assessment of risk and liability for an office facility. Allied Signal, RI, 1993.
Lloyd JD: Ergonomic assessment of risk and liability for packaging and warehouse activities. Allied Signal, Jackson Facility, TN, 1993.
Lloyd JD: Ergonomic assessment of risk and liability for furnace operators. Climax Molybdenum Company, IA, 1993.
Lloyd JD: Ergonomic assessment of risk and liability for unskilled manufacturing tasks. Climax Molybdenum Company, Langeloth Plant, PA, 1993.
Lloyd JD: Ergonomic workplace assessment and cost benefit analysis for garment manufacturing facility. Bestop Inc. – Prepared for Ergonomics Solutions Group, 1993.
Lloyd JD: Ergonomic assessment for an aftermarket product manufacturing facility. Allied Signal, UT, 1993.
Lloyd JD: Ergonomic assessment of risk and liability for sorting and packaging workstations. Allied Signal, Aftermarket Filter Division, NV, 1993.
Mitchell D, Nair C and Lloyd JD: Ergonomic assessment of risk and liability for a vehicle servicing facility. Salt River Project, Tempe, AZ, 1993.
Lloyd JD: Ergonomic assessment of risk and liability for paper manufacturing activities. Armstrong World Industries, Lancaster, PA, 1993.
Mitchell D, Costello K and Lloyd JD: Ergonomic assessment of risk and liability for gas construction and maintenance activities. Long Island Lighting Company, New York, NY, 1993.
Lloyd JD: EARLY Workplace Assessment for The Prevention of Musculoskeletal Injuries. Neapco Inc., Pottstown, PA, 1993.
Lloyd JD: Ergonomic Assessment of Risk and Liability for a Nursing Home. Presbyterian Manors, Topeka, KS, 1993.
Lloyd JD: EARLY Workplace Assessment for The Prevention of Musculoskeletal Injuries – Electronic Sales Presentation. Pioneer Electronics, CA, 1993.
Lloyd JD: EARLY Workplace Assessment for The Prevention of Musculoskeletal Injuries. American Honda Aftermarket Accessories Division, 1993.
Lloyd JD: Ergonomic Analysis of ‘The Upper Hand’ as a Tool for Reducing Physical Stress Caused by Shoveling Activities. Brookhaven National Laboratories, 1994.
Lloyd JD and Casar T: LILCO’s Ergonomics Initiative. Long Island Lighting Company, Gas Construction and Maintenance Division, New York, NY, 1994.
Lloyd JD: Corporate Ergonomics Program for Safety and Environmental Compliance. Nu-Kanu, Inc., Long Island, NY, 1994.
Lloyd JD: Training Manual for Ergonomics Laboratory. PT. Industri Pesawat Terbang Nusantara, Indonesia, 1994.
Lloyd JD: Ergonomic Analysis to Identify Physical Stressors in the Workplace. Parker-Hannifin Corporation / Gull, Hauppauge, NY; 1994.
Lloyd JD: Ergonomic Evaluation of a Hospital Emergency Reception Station with Recommendations for Redesign. John T. Mather Memorial Hospital, Port Jeff, NY; 1994.
Lloyd JD: Anthropometry – Designing for an International Population. United Airlines, CA; 1995.
Lloyd JD: Ergonomic Guidelines for Control Position and Configuration. United Airlines; 1995.
Krueger GP, Lloyd JD and Casar T: Ergonomic and Biomechanic Best-In-Class Assessment of Five .22 Caliber Rimfire and One .223 Cal Center fire Rifles. c/o Biomechanics Corporation of America, Melville, NY; 1995
Lloyd JD: Ph.D. Course in Human Factors Engineering. Kennedy-Western University; 1995
Lloyd JD: M.S. Course in Ergonomics. Kennedy-Western University; 1995.
Lloyd JD: Ergonomic Assessment of Occupational Risk Factors. Techalloy Company Welding Division, Baltimore, MD; 1995
Lloyd JD: Rapid Ergonomic Assessment of Cumulative Hazards – Hardware Loader and Hardware Unloader. Batesville Casket Company, Manchester, TN; 1995.
Gross C, Lloyd JD and Tabler R: Ergonomics Evaluation of Five Writing Instruments. Center for Product Ergonomics, University of South Florida; 1996
Lloyd JD: Demonstration of R&D capabilities for ergonomic evaluation of Harley-Davidson motorcycles. Harley-Davidson Motor Company, Milwaukee, WI; 1996
Patient Care Ergonomics Resource Guide: Safe Patient Handling and Movement. Patient Safety Center of Inquiry. October 2001
CD-ROM Interactive Training Program on Safe Patient Handling and Movement. VA Employee Education Service. 2002
Instrumented Mannequin for Restraint and Control Training: Final Report. VA Occupational Health, Washington, DC, January 2004
AORN Guidance Statement: Safe Patient Handling and Movement in the Perioperative Setting. AORN (Association of periOperative Registered Nurses), Denver, CO; 2007
Harrow JJ, Lloyd JD, Gironda R, Nelson A, Luther S, Schulz B, Applegarth S, Baptiste A and Cresta T. Final Report – Clinical Biomechanics of Wheelchair Transfers in Spinal Cord Injury: A Pilot Study. Report # B2900P. VA Rehabilitation Research and Development Service, Washington, DC; 2007
Lloyd, JD. Tailored Medical Helmets for Specific Patient Populations and Co-Morbidities. Patient Safety Center of Inquiry, Tampa, FL; 2012
Lloyd, JD. Biomechanical Evaluation of Safe Footwear for Institutional Patients, Considering Flooring Materials and Conditions. Patient Safety Center of Inquiry, Tampa, FL; 2012
Ferguson J, Caccese V, Lloyd J. Development of Headwear to Prevent Fall-Related Injuries in Elderly Persons. NIH grant final report. 2014.
Podium Presentations
‘Ergonomics In Action’ seminar discussing the importance of workplace ergonomics. Institute of Industrial Engineers, Chapter 76. Long Island, NY, January 1994
‘Mannequin Man-Modeling and HumanCAD Training Workshop.’ Northrop Grumman Corporation. Bethpage NY, December 1994
‘Biomechanics Evaluation and Comparison of Two Pole Climbing.’ Long Island Lighting Company, Hicksville, NY, September 1995.
‘Introduction to the Center for Product Ergonomics’ NASA Occupational Health Group, Kennedy Space Center, FL; May 1996.
‘Ergonomics Applications in Space’ Bayonet Point Hospital, FL; July 1996.
‘Beyond Bricks and Mortar – Innovations for Senior Living: Ergo-House.’ West Central Florida Area Agency on Aging conference; September 17, 1996.
‘Ergonomics in Action!’ ITESM International Conference, Mexico City; September 24, 1996.
‘Applied Ergonomics in Flightdeck Design’ ITESM International Conference, Mexico City; September 25, 1996.
‘Ergonomics Applications in Space’ Department of Environmental and Occupational Health, University of South Florida; October 1996.
‘Research Basis for the Development of a Dynamic Median Nerve Stress Test’ American Occupational Health Conference, Orlando, FL; May 16, 1997.
Grand Rounds: ‘Ergonomic applications for Spinal Cord Injury patients’ James A. Haley Veterans Hospital, Tampa, FL; May 23, 1997.
‘Product Ergonomics’ OSHA Regional Conference, Clearwater, FL; July 16, 1997.
‘Elderly falling study’. USF Institute on Aging Annual Meeting, Tampa, FL; April 24, 1998.
‘Etiology of musculoskeletal disorders’. Prevention of Musculoskeletal Injuries in Healthcare Workers: State of the Science. Tampa, FL; May 14, 1998.
‘Breakthrough research in injury prevention: What technology has to offer’. Prevention of Musculoskeletal Injuries in Healthcare Workers: State of the Science. Tampa, FL; May 15, 1998.
‘Ergonomic Risk Factors in the Workplace.’ Occupational Health and Safety Administration (OSHA), Tampa, FL; February 18, 1999.
‘Introduction to the 3D Static Strength Prediction Model’. National Aeronautical and Space Administration (NASA), Kennedy Space Center, FL; May 14, 1999.
‘How to Evaluate Ergonomic Products’. National Aeronautical and Space Administration (NASA), Kennedy Space Center, FL; May 14, 1999.
‘Repetitive wrist movements: an adverse effect on median nerve conduction’. American Society for Surgery of the Hand (ASSH). 54th Annual Meeting, Boston, MA; September 1999.
‘VA Biomechanics Research Laboratory – Virtual Tour’. James A. Haley Veteran’s Hospital, Patient Safety Center Press-Day. November 15, 1999.
‘Patient Safety Center of Inquiry – Technology Innovations Division’. US GAO. March 29, 2000.
‘Work-related carpal tunnel syndrome’. Alabama Governor’s safety and health conference. August 29, 2000.
‘Factors contributing to injuries related to patient handling’. VISN 8 PSCI Safe Patient Handling Conference. January 8-10, 2001.
‘Criteria for evaluating and selecting safe patient care equipment’. VISN 8 PSCI Safe Patient Handling conference, St. Petersburg Beach, FL; January 8-10, 2001.
‘Redesigning At Risk Tasks: A Panel Discussion., Safe Patient Handling and Movement conference. St. Petersburg Beach, FL; January 8-10, 2001.
Satellite Broadcasts on Safe Patient Handling and Movement. A two part series (4 hours) held August 2001 and repeated in November 2001. Part I includes the Ergonomic Workplace Assessment Protocol for Patient Care Areas. Part II includes Selecting the Right Equipment, Patient Assessment Criteria, Algorithms, and Use of Back Injury Resource Nurses.
‘New and Emerging Technology for Safe Patient Handling and Movement’ VISN 8 PSCI Safe Patient Handling Conference, Clearwater, FL; January 16-18, 2002.
‘Biomechanics Research Laboratory: A Virtual Tour’ VISN 8 PSCI Safe Patient Handling Conference, Clearwater, FL; January 16-18, 2002.
‘Biomechanical Evaluation of Friction Reducing Devices.’ James A. Haley Veterans Hospital Research Day, Tampa, FL; April 25, 2002.
‘Evaluation of Technology to Support Safe Patient Handling and Movement.’ Safe Patient Handling and Movement Conference, Clearwater, FL; March 4-7, 2003.
‘Ergonomic Comparison of Overhead Ceiling Lifts and Mobile Floor Lifts’ VISN 8 PSCI Safe Patient Handling Conference, Clearwater, FL; March 4-7, 2003.
‘New Directions in Technology for Safe Patient Handling and Movement’ VISN 8 PSCI Safe Patient Handling Conference, Clearwater, FL; March 4-7, 2003.
‘Clinical Applications in Rehabilitation Engineering’ University of South Florida MS Rehabilitation Engineering program July 2, 2003.
’Injury Epidemiology and Prevention’ University of South Florida MPH Program. August 9, 2003.
‘Biomechanical Assessment of Pressure-Relief and Repositioning Tasks in Persons with SCI’ AASCIN Conference, Las Vegas, NV; September 2005.
‘Biomechanical Evaluation of Patient Transport Technologies’ Safe Patient Handling and Movement Conference. St. Petersburg, FL; 2006.
‘Development of an Intelligent Mannequin for Research in Safe Patient Handling and Movement’ Safe Patient Handling and Movement Conference. St. Petersburg, FL; 2006.
‘Biomechanical Evaluation of Injury Severity Associated with Patient Falls from Bed’ Evidence-Based Falls Prevention Conference. St. Petersburg, FL; 2006.
‘Biomechanical Assessment of Independent Wheelchair Transfers in SCI’ AASCIN Conference, Las Vegas, NV; September 2006.
‘Lateral Patient Transfer using a Friction Reducing Device’. November 2006.
‘Vertical Patient Transfer using a Ceiling-mounted Full-Body Lift System’. November 2006.
‘Bed to Chair Transfer using a Powered Stand-Assist Lift’. November 2006.
‘Vertical Patient Transfer using a Floor-Based Full-Body Sling Lift’. November 2006.
‘Coefficient of Friction: The Science of Slips, Trips and Falls’. Florida Justice Association. February 2007.
‘Safe Patient Handling in Operating Rooms’. Safe Patient Handling and Movement Conference. Orlando, FL; 2008.
‘Biomechanical Evaluation of Patient Transport Tasks’. Safe Patient Handling and Movement Conference. Orlando, FL; 2008.
‘Car Transfer Technologies’. Safe Patient Handling and Movement Conference. Orlando, FL; 2008.
‘Evaluation of Friction Reducing Devices’. Safe Patient Handling and Movement Conference. Orlando, FL; 2008.
‘Biomechanical Evaluation of Protective Technologies for Fall Injury Prevention’. Evidence-Based Falls Prevention Conference. Clearwater, FL; 2008.
‘Development of Evidence- Based Algorithms for Safe Patient Handling of Orthopedic Patients’. Invited paper presentation at the Sigma Theta Tau International Honor Society of Nursing, 19th International Nursing Research Congress, Singapore. 2008. (presented on behalf of project team by M. Doheny)
Risks and solutions for safe patient handling in operating rooms. 9th Annual Safe Patient Handling and Movement Conference. Orlando. April 2009.
‘Transfer and Transport: Emerging technology and protocols for safe interdepartmental patient handling’. 9th Annual Safe Patient Handling and Movement Conference. Orlando. April 2009.
‘Helmet technology to minimize head injuries associated with falls’. 10th Annual Conference on Transforming Fall Management Prevention Practices. Clearwater, FL; May 2009.
‘Commercially available mats to prevent bed-related fall injuries’. 10th Annual Conference on Transforming Fall Management Prevention Practices. Clearwater, FL; May 2009.
‘Biomechanics of Traumatic Brain Injury’. Florida Public Defender’s ‘Life Over Death’ Annual Meeting. Naples, FL 2010
‘Technology Gaps Associated with Safe Patient Handling and Movement’. 11th Annual Safe Patient Handling and Movement Conference. Orlando. April 2011.
‘Biomechanics of Pediatric Brain Injury’. Department of Children and Families, Wildwood, FL. July 2012
‘Biomechanics of Pediatric Brain Injury’. Evidence Based Medicine and Social Investigation conference, Vancouver, Canada. August 3, 2012
‘Developing Helmet Standards and Testing Methods to Protect from Brain Injury’. Proceedings of the ASTM Symposium on Concussion in Sports. Atlanta, GA. November 20, 2012
‘Biomechanics of Pediatric Brain Injury’. Presented at Department of Office of the Public Defender, 13th Judicial Circuit, Tampa, FL. January 2013
‘Biomechanics of Inflicted Head Trauma’. Presented at 4th Penn State Hershey International Conference on Pediatric Abusive Head Trauma, June 27-28, 2013, Burlington, VT.
Lloyd J. BRAINS Researchers Reveal Deficiencies in Football Helmet Design (0060) 11th Annual Conference on Brain Injury. September 18-21, 2013. New Orleans, LA.
Lloyd J. Biomechanical Evaluation of Head Kinematics During Infant Shaking Versus Pediatric Activities of Daily Living. 11th Annual Conference on Brain Injury (0070). September 18-21, 2013. New Orleans, LA.
Lloyd J. Biomechanics of Brain Injuries Associated with Short Falls in Children (0072). 11th Annual Conference on Brain Injury. September 18-21, 2013. New Orleans, LA.
Lloyd J. Using LabVIEW to Design and Evaluate a Better Football Helmet. Tampabay LabVIEW users group meeting, May 21st, 2014. Tampa, FL.
Lloyd J. Using LabVIEW and Compact DAQ for Brain Injury Research. NI week keynote presentation, August 5th, 2014. Austin, TX.
Lloyd J. Using LabVIEW to Design and Evaluate a Better Football Helmet. NI week, August 7th, 2014. Austin, TX.
Lloyd J. Mechanisms of Head and Brain Injury. Manasota Trial Lawyers Association meeting. August 27, 2014
Lloyd JD. Biomechanics of Pediatric Head and Brain Trauma. Death is Different. February 20th, 2015. Orlando, FL.
Lloyd J. Brain Injury in Sports. North American Brain Injury Society 13th Annual Conference on Brain Injury. April 8th, 2016. Tampa, FL
Lloyd J. Biomechanical and Forensic Considerations of Pediatric Head Injury. Juvenile Law Dependency and Delinquency. Hosted by Florida Office of Criminal Conflict. Lake Mary, FL. June 8, 2017.
Lloyd J. Accident Reconstruction and Human Risk Factors in Driver-Impaired Crashes. Hosted by Florida Bar Association, Masters of DUI seminar. Fort Lauderdale, FL. April 5, 2019.
Lloyd J. Distracted Driving: Causes and Consequences. IPTM Symposium on Traffic Safety. June 22, 2021.
Lloyd J. Distracted Driving. WATAI Symposium on Human Factors. October 26, 2021.
Lloyd J. Lead Vehicle Looming Crashes. WATAI Symposium on Human Factors. October 27, 2021.
Lloyd J. Human Factors of Driving: Should We Be Allowed to Drive? WATAI Symposium on Human Factors. October 27, 2021.
Lloyd J. Injury Biomechanics for the Accident Reconstructionist. WREX. April 19, 2023.
Lloyd J & Forte M. Invesigating the How and Why of Motorcycle Accidents. FDLA. February 28, 2024.
Poster Presentations
‘Biomechanical assessment and stress test of dynamic postural sway to predict falls in healthy elderly’ Research Day, James A. Haley Veteran’s Hospital, Tampa, FL; April 15, 1998.
‘Effect of wrist exposures on median nerve conduction’ Research Day, James A. Haley Veteran’s Hospital, Tampa, FL; April 15, 1998.
‘A Flick of the Wrist’. University of South Florida President’s Council fundraising dinner. Tampa, FL; September 1998.
‘Repetitive wrist movements: an adverse effect on the median nerve’. University of South Florida Health Sciences Research Day. Tampa, FL; February 25, 1999.
‘Neurovascular considerations of median nerve neuropathy and implications for clinical diagnosis’. American Society for Surgery of the Hand (ASSH). 54th Annual Meeting, Boston, MA; September 1999.
‘Safe Patient Room of the Future.’ James A. Haley Veterans Hospital Research Day, Tampa, FL; April 25, 2002.
‘Stretcher Lift Design and Prototype.’ James A. Haley Veterans Hospital Research Day, Tampa, FL; April 25, 2002.
‘Whole-Body Biomechanical Model for Dynamic Analysis of Human Motion’ James A. Haley Veterans Hospital Research Day, Tampa, FL; April 29, 2005.
‘Biomechanical Evaluation of Patient Falls from Bed’. Evidenced-Based Strategies for Patient Falls and Wandering, Clearwater, FL; May 2005.
‘Estimation, Simulation, and Experimentation of a Fall from Bed’ 8th Annual Conference on Fall Prevention Strategies, Clearwater, FL; April 2007.
‘Estimation, Simulation, and Experimentation of a Fall from Bed’ James A. Haley Veterans Hospital Research Day, Tampa, FL; May 2007.
‘Evaluation of Fall Protection and Prevention Technologies’. 8th Annual Conference on Fall Prevention Strategies. Clearwater, FL; April 2007.
‘Estimation, Simulation, and Experimentation of a Fall from Bed’. 9th Annual Conference on Fall Prevention Strategies. Clearwater, FL; April 2007.
‘Biomechanical evaluation of the LiftSeat for independent patient toileting tasks’. 9th Annual Safe Patient Handling and Movement Conference. Orlando. April 2009.
‘The effects of everyday concurrent tasks on 3D overground minimum toe clearance and gait parameters’. 10th Annual Conference on Transforming Fall Management Prevention Practices. Clearwater, FL; May 2009.
‘Impact Testing to Evaluate Materials for Head Protection Devices’. 10th Annual Conference on Transforming Fall Management Prevention Practices. Clearwater, FL; May 2009.
‘Toward a Cadeveric Biomechanical Understanding of Brain Kinematics Associated with TBI’. JAHVA Research Day, 2011
‘VHA Trends in the total costs of care for the polytrauma cohort: Disproportionate impact of post-acute inpatient care’. Federal Interagency Conference on Traumatic Brain Injury, 2011
‘Toward Biomechanical Understanding of Brain Kinematics Associated with TBI using cadaveric specimens’. Federal Interagency Conference on Traumatic Brain Injury, 2011
‘Do Ill-Fitting Helmets Amplify the Risk of Head Injury Among Youth Football Players? – a Biomechanical Analysis, with Discussion for Applicability to Military Protection’. Federal Interagency Conference on Traumatic Brain Injury, 2011
‘Do Helmets Prevent Concussion?’ 8th Annual Conference of Blast Traumatic Brain Injury, December 2011, Tampa.
‘Biomechanics of Blast TBI’. 8th Annual Conference of Blast Traumatic Brain Injury, December 2011, Tampa.
‘Tampa VA Brains Researchers Reveal Deficiencies in Helmet Design’. Military Health Systems Review Symposium. August 2013, Fort Lauderdale, FL
‘How Well Do Football Helmets Protect Against Concussion and Brain Injury? American Academy of Neurology. April 30th, 2014. Philadelphia, PA.
EEG of Concussive Impact in Football. American Academy of Sports Neurology Sports Concussion meeting, July 2014. Chicago.
Military Helmets May Provide Little Protection Against Traumatic Brain Injury. Military Health Systems Research Symposium. August 2014. Ft. Lauderdale.
Lloyd JD & Conidi FX. Biomechanical Evaluation of Helmet Protection Against Concussion and TBI. International State-of-the-Science Meeting on the Biomedical Basis for Mild Traumatic Brain Injury (mTBI) Environmental Sensor Threshold Values. November 2014. MacLean, VA.
Lloyd JD, Sabbagh J & Dickey C. Investigating the Effects of Mild Blast Injury on TBI Symptoms and Tau Pathology. International State-of-the-Science Meeting on the Biomedical Basis for Mild Traumatic Brain Injury (mTBI) Environmental Sensor Threshold Values. November 2014. MacLean, VA.
Lloyd JD & Conidi FX. Do Football Helmet Add-Ons Reduce Concussion Risk? American Academy of Neurology Annual Meeting. April 2015. Washington, DC
Conferences Attended
West Central Florida Area Agency on Aging conference; September 17, 1996.
ITESM International Conference, Mexico City; September 24, 1996.
American Occupational Health Conference, Orlando, FL; May 16, 1997.
OSHA Regional Conference, Clearwater, FL; July 16, 1997.James A. Haley Veterans Hospital Research Day, FL; April 15, 1998.
Prevention of Musculoskeletal Injuries in Healthcare Workers: State of the Science. Tampa, FL; May 15, 1998
University of South Florida Health Sciences Research Day. Tampa, FL; February 25, 1999.
Alabama Governor’s safety and health conference. August 29, 2000.
VISN 8 PSCI Safe Patient Handling Conference, St. Petersburg Beach, FL; January 8-10, 2001.
Evidenced-Based Strategies for Patient Falls and Wandering, Clearwater, FL; May 2005.
AASCIN Conference, Las Vegas, NV; September 2005.
Safe Patient Handling and Movement Conference. St. Petersburg, FL; 2006.
Evidence-Based Falls Prevention Conference. St. Petersburg, FL; 2006.
AASCIN Conference, Las Vegas, NV; September 2006.
James A. Haley Veterans Hospital Research Day, Tampa, FL; May 2007.
8th Annual Conference on Fall Prevention Strategies. Clearwater, FL; April 2007.
Florida Justice Association. February 2007.
8th Annual Safe Patient Handling and Movement Conference. Orlando, FL; 2008.
9th Annual Safe Patient Handling and Movement Conference. Orlando. April 2009.
10th Annual Conference on Transforming Fall Management Prevention Practices. Clearwater, FL; May 2009.
Florida Public Defender’s ‘Life Over Death’ Annual Meeting. Naples, FL September 2010
American Academy of Forensic Sciences meeting, Chicago, IL. February 2011.
Introduction to the STAR Helmet Rating System. Virginia Tech, Blacksburg, VA. 2011.
11th Annual Safe Patient Handling and Movement Conference. Orlando. April 2011.
James A. Haley Veterans Hospital Research Day, Tampa, FL; May 2011.
Federal Interagency Conference on Traumatic Brain Injury, 2011
8th Annual Conference of Blast Traumatic Brain Injury, Tampa, December 2011
James A. Haley Veterans Hospital Research Day, Tampa, FL; May 2012.
Evidence Based Medicine and Social Investigation conference, Vancouver, Canada. August 3, 2012
New Orleans, LA. October 13-17, 2012
Special Operation Medical Association / Blast Traumatic Brain Injury, Tampa, December 2012.
American Academy of Forensic Sciences, Washington, DC. February 2013.
4th Penn State Hershey International Conference on Pediatric Abusive Head Trauma, June 27-28, 2013, Burlington, VT.
North American Brain Injury Society 11th Annual Conference on Brain Injury. September 18-21, 2013. New Orleans, LA.
North American Brain Injury Society 26th Annual Conference on Legal Issues in Brain Injury. September 18-21, 2013. New Orleans, LA.
American Academy of Neurology 66th annual meeting. April 28-May 2, 2014. Philadelphia, PA.
American Academy of Sports Neurology Sports Concussion meeting, July 2014. Chicago.
NI week. August 3-7, 2014. Austin, TX.
Military Health Systems Research Symposium. August 2014. Fort Lauderdale, FL.
International State-of-the-Science Meeting on the Biomedical Basis for Mild Traumatic Brain Injury (mTBI) Environmental Sensor Threshold Values. November 2014. MacLean, VA.
Engineering Dynamic Corporation Accident Reconstruction Course. November 10-14. Miami, FL.
American Academy of Forensic Sciences annual meeting. February 2015. Orlando, FL.
Florida Association of Criminal Defense Lawyers. Death is Different XXI. February 2015. Orlando, FL.
SAE International, April 2015. Detroit, MI.
National SBIR conference. June 15-17. National Harbor, MD.
ASTM International F08 meeting. November, 2015. Orlando, FL
North American Brain Injury Society 13th Annual Conference on Brain Injury. April 7-9, 2016. Tampa, FL.
World Reconstruction Exposition. May 2-6, 2016. Orlando, FL
National Neurotrauma Annual Meeting. June 26-29, 2016. Lexington, KY.
ASTM International F08 meeting. November 13-18, 2016. Orlando, FL
American Academy of Forensic Sciences annual meeting. February 2017. New Orleans, LA.
Juvenile Law Dependency and Delinquency. Hosted by Florida Office of Criminal Conflict. June 8-9, 2017. Lake Mary, FL.
ARC-CSI Accident Reconstruction Conference. September 18-21. Las Vegas, NV.
IPTM Symposium on Traffic Safety. May 21-24, 2018. Orlando, FL
IPTM Symposium on Traffic Safety. June 3-6, 2019. Orlando, FL
American Society of Biomechanics Virtual Annual Conference. August 3-7, 2020.
American Academy of Forensic Sciences Virtual Annual Conference. February 15-19, 2021
IPTM Symposium on Traffic Safety. June 21-24, 2021. Orlando, FL.
Pix4D conference. October 12-13, 2022. Denver, CO.
WREX 2023. World Reconstruction Exposition. April 17-21, 2023. Orlando, FL
Teaching Activities – – Graduate Students Supervised
Robert Wilson, MS; USF Department of Electrical Engineering; 1998 – ‘Occupant trajectory determinant for vehicles equipped with airbag protection systems’
Brian Waldron, BS; USF Department of Mechanical Engineering; 2000/1 ‘Engineering evaluation and modeling of harness design in full-body sling lifts’ – served as mentor for MS thesis
Oneida Westhoff, MS; USF Department of Electrical Engineering; 2003 ‘Development of an Instrumented Mannequin for Safe Patient Handling and Movement’ – served as mentor and Professor on thesis committee
Tony Cresta, MS; USF Department of Biomedical Engineering; 2003-6 ‘Biomechanical evaluation of independent transfers and pressure relief tasks in persons with SCI’ – served as mentor and Professor on thesis committee
Sruthi Vasudev Boda, MS; USF Department of Biomedical Engineering; 2003 ‘Clinical evaluation of friction reducing devices for lateral transfer of patients’ – served as mentor and Professor on thesis committee
Roberto Guerra, BS: USF Department of Electrical Engineering; 2004 ‘Development of an Instrumented Mannequin for Personal Safety Training’
Tony Morreli, BS: USF Department of Electrical Engineering; 2004 – ‘Development of an Instrumented Mannequin for Personal Safety Training’
Bonnie Bowers, MS; USF Department of Biomedical Engineering; 2004/5 ‘Biomechanics of Injuries Associated with Falls from Bed’ – served as mentor and co-Major Professor on thesis committee
Fariba Vesali, MD; USF College of Medicine; 2004 ‘Biomechanical assessment of wheelchair transfers in persons with spinal cord injury’ – served as mentor for Medical residency program
Maria Symeonidis; USF Department of Electrical Engineering; 2004 ‘Biomechanics of Injuries Associated with Falls from Bed’
Jeffrey Harrow, PhD, MD; 2006 – served as mentor for Career Development Award
Brian Schulz, PhD; 2007 – served as mentor for Career Development Award
Shawn Applegarth, PhD (c); USF Department of Mechanical Engineering; 2006 – served as mentor for PhD dissertation in biomedical engineering
Karthick Nateson; USF Department of Biomedical Engineering; 2018-9. ‘Comparison of Laboratory and Field Data Acquisition Devices for Human Activity Recording’ – served as a mentor and Professor on thesis committee
Jason Anderson; USF Department of Biomedical Engineering; 2020. ‘Psychology / Biomechanics of Falls Down Stairs’ – mentor and Co-Professor on thesis committee.
Intellectual Property Developed
Automotive Deceleration Indicator. Filed with USF Patents and Licensing office, 4/97.
Automotive Audible Warning (Horn) Intensity Controller. Filed with USF Patents and Licensing office, 4/97.
Determination of Occupant Trajectory in Airbag Protection Systems. Filed with USF Patents and Licensing office, 5/97.
Airbag Deployment Directional Controller. Filed with USF Patents and Licensing office, 5/97. Patent application # WO2001044026A1 published 6/2001. Full patent not pursued.
Airbag Depowerment Strategy as a Function of Impact Vector and Inertial Characteristics. Filed with USF Patents and Licensing office, 6/97.
CPE USF Trademark / Service Mark / Certification Mark for display on ergonomically superior products. Filed with USF Patents and Licensing office, 7/97.
Integrated vehicular security and personal assistance system. Filed with USF Patents and Licensing office, 10/97.
Orthotic device to improve blood circulation in the median distribution of the hand. Filed with USF Patents and Licensing office, 3/98.
Swimming pool feedback eyeball / diverter switch. Filed with USF Patents and Licensing office, 3/98.
Method for biomechanical evaluation of joint kinematics. Filed with Department of Veteran’s Affairs patents and licensing office, 11/99.
Integrated sling for patient lift manipulation. Filed with Department of Veteran’s Affairs patents and licensing office, 11/99.
Technology improvement for air-assisted lateral transfer devices. Filed with Department of Veteran’s Affairs patents and licensing office, 7/02.
Lateral Transfer Accessory. Patent awarded 10/3/06. # 7,114,203
Limb Holding Device. Filed with Department of Veteran’s Affairs patents and licensing office, 09/06.
Cerebral Stress Test for Objective Measurement of Brain Performance. Provisional Patent Application #61841612. 07/13. Full patent not pursued.
Materials and their Application for Protection from Traumatic Brain Injury. Provisional Patent Application #61943488. 02/14. Full patent not pursued.
Impact Absorbing Composite Material. Full US Patent Application. 05/14. Abandoned.
Mathematical Method for Analysis of Helmet Protection Against Head and Brain Injury – filed with US Copyright Office 10/15. Abandoned.
Dr. Lloyd is a distinguished authority in motorcycle accident reconstruction and human factors analysis, with decades of experience. His understanding of the unique dynamics involved in motorcycle crashes sets him apart as a true specialist in the field.
Dr. Lloyd spent his career as a senior researcher at the VA Hospital in Tampa, FL, serving as Director of the Biomechanics Research Laboratory and Director of the Traumatic Brain Injury Research Laboratory. In addition he held a courtesy faculty appointment as Assistant Professor in the University of South Florida College of Engineering from 2002-2022, and is currently the Research Director of BRAINS, Inc.
To date, Dr. Lloyd’s work has been published in six book chapters and 33 peer-reviewed journals, as well as presented at more than 100 national and international conferences (see curriculum vitae).
Comprehensive Approach
Dr. Lloyd goes beyond the obvious and delves deep into the technical intricacies of each case. As a multi-disciplinary expert he combines, accident reconstruction, biomechanics and human factors to provide a holistic view of the accident, ensuring no detail goes unanalyzed.
Accurate Reconstructions
Using state-of-the-science reconstruction tools and real world data, Dr. Lloyd meticulously creates 3D accident reconstructions with unparalleled accuracy. This empowers him to provide precise insights into the sequence of events leading up to the incident.
Human Factors Insight
Understanding the role of human behavior is crucial in accident analysis. Dr. Lloyd’s human factors expertise allows him to investigate the cognitive factors affecting both motorcycle riders and automobile drivers, offering invaluable insights into decision-making processes.
Courtroom Excellence
Dr. Lloyd’s reputation as a credible and authoritative expert makes him an invaluable asset in the courtroom. He excels at conveying complex technical information to the jury in an accessible manner, helping you present a compelling case, backed by robust scientific analysis.
To date, Dr. Lloyd has provided expert witness Deposition and Trial Testimony in more than 160 civil and criminal cases. His expertise in motorcycle crashes, motorcycle riding and operation, helmet protection, biomechanics and human factors has been recognized by courts across the United States and Internationally. The analysis methods that Dr. Lloyd utilizes are published in peer-reviewed scientific journals.
Tailored Solutions
Every case is unique. Dr. Lloyd will work closely with your legal team to tailor our services to your specific needs. Whether you required a comprehensive reconstruction, expert testimony, or consultation on specific aspects, we’ve got you covered.
Timely and Efficient
We understand the importance of time in legal proceedings. Our efficient processes ensure that you receive the insights and report you need within the necessary timelines, enabling you to proceed with your case smoothly.
Unquestionable Integrity
Ethics and integrity are the cornerstones of our practice. You can trust that our analyses are unbiased, objective and founded on the highest standards of professionalism.
Contact
Please call Dr. Lloyd at 813-624-8986 or email DrJohnLloyd@Tampabay.RR.com to discuss how he can be of help to you with your case.
Alabama Alaska Arizona Arkansas California Colorado Connecticut Delaware Florida Georgia Hawaii Idaho Illinois Indiana Iowa Kansas Kentucky Louisiana Maine Maryland Massachusetts Michigan Minnesota Mississippi Missouri Montana Nebraska Nevada New Hampshire New Jersey New Mexico New York North Carolina North Dakota Ohio Oklahoma Oregon Pennsylvania Puerto Rico Rhode Island South Carolina South Dakota Tennessee Texas Utah Vermont Virginia Washington West Virginia Wisconsin Wyoming
* peer-reviewed and published in the Journal of Forensic Biomechanics, October 2017 ** DOWNLOAD PDF FILE
Abstract
Motorcycle accident victims worldwide account for more than 340,000 fatalities annually, with the Unites States ranking 8th highest in number of motorcycle accident deaths, largely due to non-mandatory motorcycle helmet requirements for adults in a number of States. Seventy-five percent of all fatal motorcycle accidents involve head and brain injury, with rotational forces acting on the brain the primary cause of mortality. Current motorcycle helmets are reasonably effective at reducing head injuries associated with blunt impact. However, the mechanism of traumatic brain injury is biomechanically very different from that associated with focal head injury. This study was conducted to evaluate the effectiveness of current motorcycle helmets at reducing the risk of traumatic brain injuries.
Ten motorcycle helmet designs, including full-face, three-quarter and half-helmets were evaluated at an average impact velocity of 8.3 ms-1 (18.5 mph) using a validated test apparatus outfitted with a crash test dummy head and neck. Sensors at the center of mass of the headform enabled high-speed data acquisition of linear and angular head kinematics associated with impact.
Results indicate that none of the standard helmet models tested provide adequate protection against concussion and severe traumatic brain injuries at moderate impact speeds. Only one of the standard motorcycle helmet models tested provided adequate protection against skull fracture.
A new motorcycle helmet prototype, incorporating a liner constructed from a composite matrix of rate-dependent materials was tested, with comparison to standard motorcycle helmet designs, with very promising results. Knowledge learned from this study will facilitate the development of a new generation of advanced motorcycle helmets that offer improved protection against both head and brain injuries.
In developing countries motorcycles are required for utilitarian purposes due to lower prices and greater fuel economy, whereas in the developed world they are considered a luxury and used mostly for recreation. In 2016 there were more than 134 million motorcycles worldwide [1], 8.4 million of which were registered in the United States, representing 3.2% of all US registered vehicles. California, Florida and Texas were the leading states in terms of the motorcycle popularity; collectively representing 22% of all US registered motorcycles [2]. In 2011, U.S. motorcyclists travelled a total of 18.5 billion miles, which, while only 0.6% of total vehicle miles travelled, accounted for 14.6% (4,612) of U.S. traffic fatalities that year. Worldwide there are more than 340,000 motorcyclist fatalities annually, which equates to more than 28% of all road accident deaths [3]. According to the U.S. National Highway Traffic Safety Administration (NHTSA) and other reports, when compared per vehicle mile traveled with automobiles, due to their vulnerability, motorcyclists’ risk of a fatal crash is 30-35 times greater than that of a car occupant [4][5][6][7].
Two fundamental epidemiologic studies into the causation of motorcycle accidents have been conducted: the Hurt study in North America and the MAIDS study in Europe. According to the Hurt Report [8], 75 percent of collisions were found to involve a motorcycle and a passenger vehicle, while the remaining 25% were single vehicle accidents. The cause of motorcycle versus passenger vehicle collisions in 66% of accidents involves violation of the rider’s right of way due to the failure of motorists to detect and recognize motorcycles in traffic. Findings further indicate that severity of injury to the rider increases with alcohol consumption, motorcycle size and speed.
The most recent epidemiologic study to investigate motorcycle accident exposure data was conducted between 1999-2001 by a partnership of five European countries [9]. Findings show that passenger cars were again the most frequent collision partner (60%), where more than two-thirds of drivers reported that they did not see the motorcycle and more than half of all accidents involving motorcycles occurred at an intersection.
The COST report, which is an extension of the MAIDS study, documents that three-quarters (75%) of all motorcyclist deaths are a result of injury to the head and brain [10]. Linear forces were the major factor in 31% of fatal head injuries, while rotational forces were found to be the primary cause in over 60% of cases. While the helmet is considered the most effective means of rider protection [11], recent studies indicate that motorcycle helmets are only 37-42% successful in preventing fatal injury [12],[13]. By reducing peak linear forces acting on the head it was commonly believed that the risk of diffuse brain injuries, including concussion, subdural hematoma and diffuse axonal injury would also be prevented [8]. However, the biomechanical mechanisms of head and brain injuries are unique. New research shows that these mechanisms are poorly correlated [14].
Motorcycle Helmet Standards
Like most helmets, motorcycle helmets are modeled after ancient military helmets, the purpose of which is to provide protection against penetrating head injury, such as skull fracture. Whereas, all impacts have both linear and oblique components, which produce translational and tangential forces, respectively. The modern motorcycle helmet was introduced over 60 years ago [15]. Its outer shell serves as a second skull, diffusing impact forces over a larger surface area, while the inner liner compresses to minimize translational forces. However, a mechanism to mitigate tangential forces is absent. Since the liner fills the entire inner surface of the shell and is immobile, rotational inertia induced tangential forces are transmitted directly to the brain.
The likelihood of a helmeted motorcyclist sustaining impact loading injuries, such as skull fractures, can be determined by quantifying the magnitude of peak linear acceleration experienced by a test headform in response to impact. Whereas the risk of a rider suffering inertial or impulse loading injuries, such as concussion, axonal injury and intracranial hematoma can be computed based on impact-related angular kinematics at the headform center of mass [16],[17].
Unfortunately motorcycle helmet protection is not driven, for the most part, by advances in scientific knowledge, but by the need to meet applicable testing standards [18],[19]. In the United States, the governing specification is the federal motor vehicle safety standard (FMVSS) #218 [20]; the Snell Memorial Foundation also offers a voluntary standard M2015, which is a little more stringent [21]. Whereas BSI 6658 [22] and ECE 22.05 [23] have been adopted in European countries and AS/NZS 1698 accepted in Australasian countries [24]. Test protocols involve the guided fall of a helmeted headform onto steel anvils of various designs at impact velocities ranging from only 5.2 to 7.5 m/s (11-17 mph). The pass/fail criterion is based only on the helmet’s effectiveness in reducing peak linear acceleration, and thereby translational forces, in response to impact.
Impact-related angular head kinematics are not quantified under current motorcycle helmet standards, which therefore fail to assess whether helmets offer any protection against traumatic brain injuries. The omission of this critical measure of helmet performance is reflected epidemiologically in the disproportion of closed head and brain injuries in fatal motorcycle accidents [9,10].
Biomechanics of Head and Brain Injury
The two mechanisms associated with traumatic head and brain injury are impact loading and impulse loading, both of which are present in all impact events. Impact loading involves a blow directed through the center of mass of the head, resulting in translation of the head and brain. When thresholds of injury are exceeded, skull fractures [25], lacerations and contusions (bruising) to the head and underlying brain tissue may result [26]. Whereas, impulse or inertial loading is produced when an oblique impact, common to motorcycle crashes, creates tangential forces, causing head rotation. Since the brain is not rigidly attached to the inside of the skull, rotational inertia of the brain produces a mechanical strain on cerebral blood vessels, nerve fibers and brain tissue. When thresholds of injury are exceeded, nerve fibers in the brain may be damaged, producing concussion [27] and diffuse axonal injury (DAI) [28]. Blood vessels may also rupture, causing subdural hemorrhages (SDH) [29], the high mortality rate of which has motivated numerous studies of bridging vein failure properties [30],[31],[32],[33],[34],[35]. Subdural hematoma and traumatic axonal injury are frequently identified as the cause of serious injury or fatality in motorcycle accidents.
Holbourn [[36]] was the first to identify angular / rotational acceleration as the principal mechanism in brain injury. Gennarelli, Ommaya and Thibault further investigated the importance of rotational (angular) acceleration in brain injury causation, based on studies involving live primates and physical models, [28,29,[37],[38],[39], concluding that angular acceleration is far more critical than linear acceleration to the causality of traumatic brain injuries. They further isolated and investigated the unique effects of translational (linear) and inertial (angular) loading on the heads of primates [28], confirming that pure translation produces focal injuries, such as contusions and skull fractures, while rotationally induced inertial loading causes diffuse effects, including concussion and subdural hematoma. Closed head and brain injury, found in more than 60% of motorcycle accident fatalities, is due to inadequate helmet protection against impact-related angular head kinematics [10].
Skull fracture:
Ono [25] published thresholds for human skull fracture based on cadaver experiments. Twenty-five human cadaver skulls were exposed to frontal, occipital and lateral impacts. Each skull was covered with the rubber skin of a Hybrid II mannequin and filled with gelatin to accurately represent head mass. A series of 42 frontal, 36 occipital and 58 temporal blows were delivered to the suspended heads, during which linear accelerations were measured. A skull fracture threshold of 250 g for 3-millisecond impulse duration was established for frontal and occipital impacts, decreasing to 140 g for 7-millisecond impulse duration. Whereas the skull fracture threshold for lateral impacts is reported as 120 g over 3-millisecond duration, decreasing to 90 g over 7 milliseconds. Results indicate that skull fracture threshold is inversely related to impulse duration.
Concussion:
Several studies have attempted to establish biomechanical thresholds for concussion. Pellman et al. analyzed a series of video-recorded concussive impacts during NFL football games, reporting that concussive injury is possible at 45 g / 3500 rad/s2, while 5500 rad/s2 represents a 50% risk of concussive trauma [40]. Rowson and Duma, also using head injuries in America football as their model, conducted extensive laboratory and field-based biomechanical evaluations [41],[42],[43],[44]. Based on data from 62,974 sub-concussive impacts and 37 diagnosed concussions recorded using the Simbex, Inc. (Lebanon, NH) Head Impact Telemetry System (HITS), the investigators propose a concussion threshold of 104 ± 30 g and 4726 ± 1931 rad/s2.
Subdural Hematoma:
According to Gennarelli, the most common form of acute subdural hematoma (ASDH) is caused by shearing of veins that bridge the subdural space [29]. The severity of injury associated with bridging vein rupture has led to numerous studies of their mechanical properties (Lowenhielm [30-31,32], Lee and Haut [33], Meaney [34], and Depreitere [35]).
Lowenhielm tested 22 human parasagittal bridging vein samples from 11 decedents between the ages of 13 and 87 years without history of brain injury [30,31]. He hypothesized that blunt trauma to the head causes the brain to be displaced with respect to the dura, thereby stretching bridging veins and surrounding connective tissue. Based on his laboratory experiments, Lowenhielm found that maximal shear stresses occur about 7 milliseconds after impact, coinciding with bridging vein disruption. He concluded that bridging vein rupture may occur if peak angular acceleration exceeds 4500 rad/s2.
Depreitere subjected ten unembalmed human cadavers to 18 occipital impacts producing head rotation of varying magnitude and impulse duration in the sagittal plane [35]. Bridging vein ruptures, detected by autopsy, were produced in six impact tests. Findings suggest a mean tolerance level of approximately 6,000 rad/s2 for 10-millisecond impulse duration, which seems to decrease for longer impulse durations, however the confidence interval is rather broad due to the limited data set. Data from the research by Depreitere and Lowenhielm is presented in Figure 1.
Figure 1: Bridging vein failure as a function of impulse duration and peak angular acceleration (with line of best fit and 75% confidence intervals).
Helmets decrease peak translational force by extending the impulse duration. In the case of motorcycle helmets, typical impulse duration is approximately 12 milliseconds. With reference to Figure 1, above, this suggests that bridging vein rupture may result with peak angular accelerations in the order of 5,000 rad/s2, but may be as low as 3,000 rad/s2 after adjusting for standard error of the mean in this limited dataset.
While previous studies have investigated motorcycle impacts into vehicles and fixed barriers, the underlying motivation of such studies was to determine crush characteristics of the vehicles for accident reconstruction purposes [45]. Other studies have evaluated peak linear accelerations of the head, chest and pelvis of motorcyclists in collisions [46]. However, rotational forces associated with impact-related peak angular accelerations have not been determined even though it is well known that rotational mechanisms are the primary cause of closed head injuries [28,29,36-37,38,39] in helmeted motorcyclist accidents [10]. Measurement of impact-related head angular / rotational acceleration is critical to the development and evaluation of motorcycle helmets to provide effective protection against traumatic brain injuries associated with a range of typical motorcycle crash-related head impact speeds. To that end, this paper offers an objective determination of the performance of a variety of motorcycle helmets in terms of their ability to protect against both head and traumatic brain injuries associated with impact velocities reflective of typical head impact velocities in motorcycle accidents.
Methods
The standard test apparatus for impact testing of protective headwear was modified to enable measurement of both linear and angular headform kinematics [16]. This validated apparatus is comprised of parallel vertical braided stainless steel wires that guide the fall of a 50th percentile Hybrid III head and neck assembly (HumaneticsATD, Plymouth, MI) mounted to an aluminum flyarm. The anvil onto which the headform impacts consists of a 50 mm thick steel base plate, with a 100 mm thick concrete overlay, consistent with the coefficient of friction for typical roadway surfaces. Figure 2 illustrates this setup.
Figure 2: Modified Head drop system with Hybrid III head / neck
According to Mellor et al. [47] apparatus for the evaluation of protective headgear in which the headform is rigidly affixed to the carriage (flyarm) reduces the dissipation of energy by excessive rotation of the helmeted headform and sliding of the helmet on the anvil, thereby inflating peak linear acceleration measures. Examples in which the headform is rigidly affixed to the flyarm include the FMVSS218 test apparatus [20]. Whereas in Snell M2015 [21], BS 6658 [22] and AS/NZS 1698 [24] specifications the headform is attached to the flyarm by means of a hinge joint, which allows headform rotation in the sagittal plane as well as vertical translation, but prevents motion in the coronal and axial planes. The ECE 22:05 test method [23] utilizes a ball joint between the flyarm and headform, thereby permitting unrestricted head rotation in all three planes. Similar to the ECE test method, utilization of the Hybrid III neck permits headform rotation in sagittal, coronal and axial planes, but limits the rate of motion in a manner more consistent with the human musculoskeletal system [48]. Moreover, orientation of the Hybrid III neck was maintained relative to the flyarm, irrespective of headform orientation, thereby standardizing response of the neck form.
Instrumentation: A triaxial block, installed at the center of mass of the Hybrid III headform (HumaneticsATD, Plymouth, MI) housed a triaxial accelerometer from PCB Piezotronics (Depew, NY) and three DTS-ARS Pro angular rate sensors (Diversified Technical Systems, Seal Beach, CA). Data from the sensors were acquired using compact DAQ hardware from National Instruments (Austin, TX).
While all sensors had been calibrated by the respective manufacturers, verification tests were performed to validate linear and angular sensor calibration data. Calibration of the tri-axial linear accelerometer was validated using a portable handheld shaker and found to be within specification for all three axes of measurement. For the angular rate sensor a simple validation method was devised in which the sensor was affixed to a digital goniometer, which was moved through a set angle (Figure 3). Using LabView, the integral of angular rate was computed, reflecting concurrence with the digital goniometer for all three planes of motion.
Figure 3: Validation of Angular Rate Sensor Calibration
Ten motorcycle helmet models were selected for evaluation, based on popularity among motorcyclists, including representative models of full-coverage, three-quarter and half-helmet (shorty) styles, as shown in Figure 4, below. All models displayed the DOT certification sticker, indicating that their protective performance met the FMVSS218 motorcycle helmet testing standard [20]. Helmet sizes were chosen based on best fit for the Hybrid III headform, which has a 58cm head circumference, representative of a 50th percentile US adult male.
Figure 4: Motorcycle Helmet Models Evaluated
In addition, a new prototype motorcycle helmet (Figure 5) was tested for comparison against the ten standard DOT motorcycle helmets. The prototype helmet was a three-quarter standard shell with liner constructed from a composite of rate-dependent materials arranged in a patent-pending matrix [49].
Figure 5: Motorcycle Helmet Prototype
Five samples of each motorcycle helmet model were purchased in new condition. Each helmet was impacted one time in the frontal and/or occipital region at an impact velocity of approximately 8.3 meters per second (18.5 mph), which was verified computationally. Repeatability of the tests was confirmed at the start and end of data collection by dropping the Hybrid III headform from a height of 2.0 m onto a Modular Elastomer Programmer (MEP) pad of 25 mm thickness and durometer 60A. Standard Error of the Mean of 0.061 was computed based on peak angular accelerations for pre and post MEP pad drop tests.
Analysis: Analog sensor data were acquired at 20 kHz per channel, in accordance with SAE J211 [50], using LabView (National Instruments, Austin, TX). The raw data was then filtered in MATLAB (The MathWorks, Natick, MA) using a phaseless eighth-order Butterworth filter with cutoff frequencies of 1650 Hz and 300Hz for the linear accelerometers and angular rate sensors, respectively. Angular acceleration measures were computed from the angular velocity data using 5-point least-squares quartic equations. Impulse duration was determined based on the linear acceleration signal, where impulse start point is the time at which the magnitude of linear acceleration exceeds 3 g and impulse end point is the time at which the major component of linear acceleration crosses the y-axis (Figure 6). The gradient from impulse start point to peak was computed, as was the area under the acceleration magnitude curve from start to end points. Variables for the angular acceleration signal were similarly computed.
Figure 6: Impulse duration based on linear acceleration data
An analysis method validated by Takhounts [51] establishes physical (strain and stress based) injury criteria for various types of brain injury based on scaled animal injury data and uses Anthropomorphic Test Device (ATD) test data to establish a kinematically based brain injury criterion (BrIC) for use with ATD impact testing. This method was utilized to express risk of brain injury according to the recently revised AIS scale [52] in terms of peak angular head kinematics, where:
The probability of brain injury for AIS 1-5 was thus computed as a function of BrIC:
Additionally, mechanical head and brain injury parameters of maximum pressure (in kPa), maximum principal strain (MPS) and cumulative strain damage measure (CDSM) were computed for each helmet impact test:
Results
The following table presents a summary of results for each of helmet models evaluated:
Table 1: Summary of Results
* The best performing helmet for each variable is highlighted in green
* The worst performing helmet for each variable is highlighted in red
Motorcycle Helmet Protection against Skull Fracture:
Figure 7, below, presents peak linear acceleration values, averaged across 5 samples of each of the 10 motorcycle helmet models tested, along with results for the prototype, against pass/fail thresholds for current motorcycle helmet testing standards (DOT, Snell, BS and ECE) as well as frontal-occipital and lateral skull fracture thresholds, per Ono [25].
Figure 7: Risk of Skull Fracture Associated with Motorcycle Helmet Impacts
Results show that while all of the motorcycle helmet models evaluated satisfy at least the DOT standard, only the Scorpion T510 full-face helmet offers sufficient protection against fronto-occipital and lateral impacts at the moderate impact velocities at which the helmets were tested.
Motorcycle Helmet Protection against Concussion:
Figure 8 presents peak angular acceleration results for 8.3 m/s impacts onto a concrete anvil, averaged across 5 samples of each helmet model. The red horizontal line on figure 8 indicates the 50% threshold for concussive trauma, as defined by Pellman et al [40].
Figure 8: Risk of Concussion Associated with Motorcycle Helmet Impacts
Results show that while a DOT approved motorcycle helmet may reduce peak angular acceleration associated with a helmeted head impact, the level of protection is not sufficient to prevent concussive injury in a typical motorcycle accident. Only the prototype motorcycle helmet, incorporating a liner constructed from a composite of rate-dependent materials arranged in a patent-pending matrix [49], offered adequate protection against concussive events.
Motorcycle Helmet Protection against Subdural Hematoma:
Figure 9, below, presents peak angular acceleration as a function of impulse duration, averaged across 5 samples of each of the 10 motorcycle helmet models tested, along with results for the prototype helmet. The threshold for bridging vein failure and resultant subdural hematoma is represented by the black line of best fit. Upper and lower boundary limits of this threshold are indicated in red, which represents a 75% likelihood that a subdural hematoma may occur for peak angular accelerations above the lower red line.
Figure 9: Risk of Subdural Hematoma Associated with Motorcycle Helmet Impacts
Most of the helmets tested, with exception of the prototype, fall above the lower threshold line suggesting the likelihood of catastrophic brain injury associated with a moderate helmeted impact. In fact, all but one of the five half-helmet models tested produced results above the mean threshold for subdural hematoma, indicating a higher likelihood of severe (AIS 4) or critical (AIS 5) brain injury. Overall, it appears that full-face helmets generally outperform half helmets in reducing the risk of subdural hematoma. Interestingly, an unhelmeted individual can seemingly withstand substantially greater peak angular accelerations and consequently experiences a lower risk of catastrophic brain trauma than a helmeted individual.
Correlation Analyses:
Pearson’s correlations were computed between each of the variables. Trends were suggested if computed R2 values were greater than 0.70, while strong correlations are indicated if R2 exceeded 0.80. Across all measures, the three most important variables, in rank order, for determining risk of head and brain injury are peak angular acceleration, angular acceleration gradient, and area under the angular acceleration curve between impulse start to end. The following interesting results were observed:
A negative trend exists between helmet mass and both linear acceleration (-0.70) and angular acceleration (-0.72). That is, both peak linear acceleration and peak angular acceleration seem to decrease as helmet mass increases.
There is neither a trend nor strong correlation between linear velocity and any of the variables investigated. This finding suggests that risk of head and brain injury is not related to impact speed.
A strong negative correlation exists between peak linear acceleration and impulse duration (-0.92). That is, impulse duration increases as peak linear acceleration decreases.
A trend, but not strong correlation was found between peak linear acceleration and peak angular acceleration, indicating that reducing impact-related peak linear acceleration may not necessarily mitigate peak angular acceleration.
Peak angular acceleration is strongly correlated with rotational injury criterion (RIC36) (0.95), Brain rotational Injury Criterion (BrIC) (0.93), probability of brain injury AIS 2 through 5 (μ=0.91), angular acceleration gradient (0.98), and area under the angular acceleration curve (0.96). A strong negative correlation is identified between peak angular acceleration and cumulative strain damage measure (CSDM) (-0.94) and maximum principal strain (MPS) (-0.94). A positive trend is also noted between peak angular acceleration and maximum pressure (0.77), Gadd Severity Index (GSI) (0.74) and linear acceleration gradient (0.76).
Discussion
As presented, the mechanisms associated with causation of focal head injuries and diffuse brain injuries are very different. Helmets were originally intended and continue to be designed to reduce the risk of potentially fatal head injuries caused by skull fracture fragments penetrating the brain. While skull fractures have been almost entirely eliminated in activities such as American Football, the higher impact speeds associated with motorcycle collisions continue to result in life-threatening cranial fractures, even in areas covered by the helmet. Thus, minimizing peak linear accelerations remains an important function of any motorcycle helmet. Therefore, to minimize the risk of skull fractures associated with helmeted motorcycle collision, based on research by Ono [25], a threshold of 140 g for peak linear acceleration to the frontal and occipital areas of the head and 90 g for peak linear acceleration for lateral impacts is suggested as a suitable performance criteria.
However, as with most helmets, motorcycle helmets perform inadequately in terms of mitigating the forces responsible for causing traumatic brain injury. Though a trend may exist between peak linear acceleration and peak angular acceleration, a strong correlation is absent, consistent with prior work in this area [14]. Hence, reduced peak linear acceleration through improved helmet design may not reduce the risk of traumatic brain injury. Indeed, as results herein show, an unhelmeted individual may be at a lesser risk of subdural hematoma during a moderate speed impact than one who is wearing a DOT approved motorcycle helmet.
Motorcycle Helmet Biomechanics
To minimize the risk of traumatic brain injury, spanning from mild concussion (AIS2) through severe brain injury (AIS5), it is necessary to reduce impact-related peak angular velocities in the sagittal, coronal and axial planes. Furthermore, since risk of subdural hematoma is defined based on peak angular acceleration and impulse duration, reducing peak angular velocities while also managing impulse duration will also lend to risk reduction of such severe or critical traumatic brain injuries. Therefore, to minimize the risk of concussion and subdural hematoma in helmeted motorcycle collisions, it is suggested that performance criteria based on peak angular velocity and acceleration not exceed 15.0 rad/s and 3,000 rad/s2, respectively, as previously proposed for American Football helmets [17].
Figure 10, below, was prepared to illustrate the relative effectiveness of the ten motorcycle helmet models tested and prototype in terms of protection against skull fracture, concussion and subdural hematoma, based on the above suggested performance criteria. Results indicate that only the prototype provides adequate protection against both traumatic head and brain injuries.
Figure 10: Motorcycle Helmet Effectiveness in Protecting Against Skull Fracture, Concussion and Subdural Hematoma
Based on the overall performance in terms of protection against skull fracture, concussion and subdural hematoma, and assuming equal weighting of these criteria for visualization purposes, the helmet models are presented in rank order in Figure 11.
Figure 11: Motorcycle Helmet Effectiveness (presented in rank order from left to right)
A strong negative correlation has been shown between helmet mass and both peak linear and angular accelerations. This finding suggests that ‘novelty’ motorcycle helmets (i.e. those not meeting FMVSS218 or other motorcycle helmet standards), which are often of lighter weight than DOT-approved helmets, will likely perform poorly in terms of preventing both head and brain injuries.
The new motorcycle helmet prototype evaluated within the scope of this study demonstrated exceptional potential to minimize the risk of traumatic brain injury, from mild concussion through severe brain injury, for a helmeted motorcyclist involved in a collision of moderate head impact speed.
Conclusions
The purpose of a motorcycle helmet is to reduce blunt force trauma to the head, thereby decreasing the risk of lacerations, contusions and skull fractures,. Whereas brain injuries may be produced when the brain lags behind sudden head motion thereby causing brain tissue, nerves and blood vessels to stretch and tear. The type of brain injury sustained is dependent on the magnitude and the time (pulse) duration over which mechanical stresses and strains act on the brain.
Motorcycle helmet test standards focus on reducing forces associated with linear acceleration by dropping helmeted headforms onto an anvil from a stated height and measuring the resultant peak linear acceleration. In general, the helmet design is considered acceptable if the magnitude of peak linear acceleration is less than an established threshold. Thus, helmets can and do prevent fatalities associated with penetrating head trauma. However, it may be argued that protection against brain injury is of paramount importance. After all, cuts, bruises and even bone fractures will heal, but brain injuries, if not fatal, often have life long neurologically devastating effects.
Current helmet testing standards do not require performance measures in terms of angular head kinematics and therefore fail to address whether motorcycle helmets provide the necessary protection against traumatic brain injuries. Research presented herein shows that it is possible to sustain catastrophic brain injuries, even while wearing a motorcycle helmet certified according to present testing standards.
Future generations of motorcycle helmets ought to be evaluated at higher impact velocities that are more indicative of head impact velocities in typical motorcycle accidents and should incorporate measures of both linear and angular acceleration to quantify their protective properties against both traumatic head and brain injuries.
[8] Hurt HH, Ouellet JV & Thom DR (1981) Motorcycle Accident Cause Factors and Identification of Countermeasures. Volume 1: Technical Report. Traffic Safety Center, University of Southern California, Los Angeles, CA.
[11] Chang L, Chang G, Huang J, Huang S, Liu D et al. (2003) Finite Element Analysis of the effect of motorcycle helmet materials against impact velocity. Journal of the Chinese Institute of Engineers. 26: 835–843.
[16] Caccese V, Lloyd J, Ferguson J (2014) An Impact Test Apparatus for Protective Head Wear Testing Using a Hybrid III Head-Neck Assembly. Experimental Techniques. PMID: 28216804
[17] Lloyd J & Conidi F (2015) Brain Injury in Sports. Journal of Neurosurgery. 124(3):667-74 PMID: 26473777
[22] BSI (1985) BS 6658 – Specification for protective helmets for vehicle users. British Standards Institute.
[23] ECE (2002) 22.05 Protective Helmets and their Visors for Drivers and Passengers of Motorcycles and Mopeds.
[24] Australian/New Zealand Standard (2006) AS/NZS1698, Protective Helmets for Vehicle Users. Australian/New Zealand Standard.
[25] Ono K (1998) Human head impact tolerance. In Yoganandan (Ed). Frontiers in Head and Neck Trauma: Clinical and Biomechanical. IOS Press, Amsterdam.
[26] Nahum, A. M., Gatts, J. D., Gadd, C. W., Danforth, J (1993) Impact Tolerance of the Skull and Face. In Biomechanics of Impact Injury and Injury Tolerances of the Head-Neck Complex. Ed. Stanley H. Backaitis. Warrendale: Society of Automotive Engineers. 631-645.
[28] Gennarelli TA, Thibault LE, Adams JH, Graham DI, Thompson CJ, et al (1982) Diffuse axonal injury and traumatic coma in the primate. Ann Neurol. 12(6): 564-74. PMID: 7159060
[29] Gennarelli T. and Thibault L (1982) Biomechanics of Acute Subdural Hematoma, J Trauma. 22(8), 680-686. PMID: 7108984
[30] Lowenhielm P (1974) Dynamic properties of the parasagittal bridging veins. Z. Rechtsmed. 74 (1): 55-62. PMID: 4832079
[31] Lowenhielm P (1975) Strain Tolerance of the Vv. Cerebri sup. (Bridging Veins) Calculated from Head-on Collision Tests with Cadavers. Z. Rechtsmed. 75 (2): 131-144. PMID: 4217056
[32] Lowenhielm P (1978) Tolerance level for bridging vein disruption calculated with a mathematical model. J Bioengineering. 2 (6): 501-507. PMID: 753840
[33] Lee MC and Haut RC (1989) Insensitivity of tensile failure properties of human bridging veins to strain rate: implications in biomechanics of subdural hematoma. J Biomechanics. 22 (6-7): 537–542. PMID: 2808439
[34] Meaney DF (1991) Biomechanics of acute subdural hematoma in the subhuman primate and man. University of Pennsylvania. PhD dissertation.
[38] Gennarelli TA, Adams JH, Graham DI (1981) Acceleration induced head injury in the monkey I: The model, its mechanistic and physiological correlates. Acta Neuropathol. Suppl. 7:23-25. PMID: 6939241
[39] Thibault LE and Gennarelli TA (1985) Biomechanics of diffuse brain injuries. Stapp Car Crash Conference. Twenty-Ninth Proceedings, SAE Paper No. 856022, New York.
[40] Pellman EJ, Viano DC, Tucker AM, Casson IR, Waeckerle JF (2003) Concussion in professional football: reconstruction of game impacts and injuries. Neurosurgery. 53(4): 799-812. PMID: 14519212
[41] Rowson S, Brolinson G, Goforth M, Dietter D, Duma S (2009) Linear and angular head acceleration measurements in collegiate football. J Biomech Eng. 131(6). PMID: 19449970
[42] Rowson S, Goforth MW, Dietter D, Brolinson PG, Duma SM (2009) Correlating cumulative sub-concussive head impacts in football with player performance. Biomed Sci Instrum. 45:113-8. PMID: 19369749
[43] Rowson S, Duma SM, Beckwith JG, Chu JJ, Greenwald RM, et al (2012) Rotational head kinematics in football impacts: an injury risk function for concussion. Ann Biomed Eng. 40(1): 1-13. PMID: 22012081
[44] Rowson S, Duma SM (2013) Brain injury prediction: assessing the combined probability of concussion using linear and rotational head acceleration. Ann Biomed Eng. 41(5): 873-82. PMID: 23299827
[45] Adamson KS, Alexander P, Robinson EL, Johnson GM, Burkhead CI, et al. (2002) Seventeen motorcycle crash tests into vehicles and a barrier. SAE 2002-01-0551. Society of Automotive Engineers, Warrendale, PA.
[46] Severy DM, Brink HM, Blaisdell DM (1970) Motorcycle collision experiments. SAE Technical Paper 700897. Society of Automotive Engineers, Warrendale PA.
[47] Mellor AN, St Clair VJM, Chinn BP (2007) Motorcyclists’ helmets and visors – test methods and new technologies. TRL Limited, Wokingham, Berkshire, UK. Project # S0232/VF.
[48] Mertz HJ, Patrick LM (1971) Strength and Response of the Human Neck. Stapp Car Crash Conference; SAE Technical Paper 710855. Society of Automotive Engineers, Warrendale PA.
John Lloyd of BRAINS, Inc. announced today that football head injuries and concussions can be reduced up to 50 percent with their new helmet safety breakthrough.
football helmet prototype
San Antonio, FL – Dr.John Lloyd PhD of BRAINS, Inc. announced their latest breakthrough in football helmet safety today. The unique new helmet technology promises to provide up to 50 percent more protection against football head injuries and concussions. The technology has wide application and can be used in every kind of helmet from baby helmets to military helmets, and for all athletes at risk of concussion and head injuries such as football players, cyclists, skiers, snowboarders, skateboarders, hockey players, baseball players, lacrosse players, boxers, soccer players, equestrian / horse-riding sports, such as polo and horse racing, as well as motorcycle and race car drivers.
Recent medical research documents found that concussions and cumulative head impacts can lead to lifelong neurological consequences such as chronic traumatic encephalopathy, a degenerative brain disease known as CTE and early Alzheimer’s.
The U.S. Centers for Disease Control and Prevention, estimates 1.6 – 3.8 million sport-related brain injuries annually in the United States. Of these 300,000 are attributed to youth football players, some of whom die from their injuries every year – a tragedy difficult for their mothers and families to recover from.
The severity of the issue touching both the nation’s youth and professional athletes has led to thousands of lawsuits and Congressional Hearings. Growing concern has spread to the White House where President Obama recently spoke at the Healthy Kids and Safe Sports Concussion Summit.
The BRAINS, Inc. research team, led by renowned brain injury expert, Dr. John Lloyd, has worked for years on their project to help make sports safer. A controversial subject, some opponents have stated that concussion prevention is impossible. Dedicated to saving lives and preserving brain health, Dr. Lloyd and team persevered with their work leading to this new innovation. “Our results show that forces associated with concussion and brain injury are reduced up to 50% compared to similar testing with a leading football helmet,” said Dr. John Lloyd, Research Director.
helmet prototype reduces concussion and brain injury risk
“The patent-pending matrix of non-Newtonian materials will not only benefit football, but can be utilized in all sports helmets as well as military, motorcycle and even baby helmets to improve protection and dramatically reduce the risk of brain injuries,” reported Dr. Lloyd.
The materials are inexpensive, and produce a helmet that is considerably lighter and more comfortable than a traditional helmet. Two additional applications of this new safety technology include medical flooring especially in hospitals and nursing homes or child play areas , as well as vehicle interiors.
About BRAINS, Inc.
BRAINS, Inc. located in San Antonio, Florida, is a research and development company focused on the biomechanics of brain injuries. The company was founded in 2011 by John D. Lloyd Bio, Ph.D., CPE, CBIS, Board Certified Ergonomist and Certified Brain Injury Specialist. He has also provided expert witness services nationwide for over 20 years in the fields of biomechanics, ergonomics and human factors, specializing in the biomechanics of brain injury, including sport and motorcycle helmet cases, slips and falls, motor vehicle accidents and pediatric head trauma. BRAINS, Inc. is open to licensing with manufacturers to bring this much-needed technology to market for the protection of sports participants and athletes of all ages. For additional information visit : http://drbiomechanics.com/sports-helmet-football-helmets/new-helmet-technology/ or call 813-624-8986.
Dr. John Lloyd, Research Director of Brains, Inc. announced today that football head injuries and concussions can be reduced up to 50 percent with their new helmet technology.
football helmet prototype
Tampa, FL – John Lloyd PhD, Research Director of Brains, Inc. announced their latest breakthrough in football helmet safety today. The unique new helmet technology promises to provide up to 50 percent more protection against football head injuries and concussions. The helmet technology has wide application and can be used in every kind of helmet from baby helmets to military helmets, and for all athletes at risk of concussion and head injuries such as football players, cyclists, skiers, snowboarders, skateboarders, hockey players, baseball players, lacrosse players, boxers, soccer players, equestrian / horse-riding sports, such as polo and horse racing, as well as motorcycle and race car drivers.
Recent medical research documents found that concussions and cumulative head impacts can lead to lifelong neurological consequences such as chronic traumatic encephalopathy, a degenerative brain disease known as CTE and early Alzheimer’s.
The U.S. Centers for Disease Control and Prevention, estimates 1.6 – 3.8 million sport-related brain injuries annually in the United States. Of these 300,000 are attributed to youth football players, some of whom die from their injuries every year – a tragedy difficult for their mothers and families to recover from. The severity of the issue touching both the nation’s youth and professional athletes has led to thousands of lawsuits and Congressional Hearings. Growing concern has spread to the White House where President Obama recently spoke at the Healthy Kids and Safe Sports Concussion Summit.
The BRAINS research team, led by renowned brain injury expert, Dr. John Lloyd, has worked for years on their project to help make sports safer. A controversial subject, some opponents have stated that concussion prevention is impossible. Dedicated to saving lives and preserving brain health, Dr. Lloyd and team persevered with their work leading to this new innovation. “Our results show that forces associated with concussion and brain injury are reduced more than 50% compared to similar testing with a leading football helmet,” said Dr. John Lloyd, Research Director. Results of our prototype helmet technology compared to the Riddell Revolution Speed varsity helmet are presented below: “The patent-pending matrix of non-Newtonian materials will not only benefit football, but can be utilized in all sports helmets as well as military, motorcycle and even baby helmets to improve protection and dramatically reduce the risk of brain injuries,” reported Dr. Lloyd. The materials are inexpensive, and produce a helmet that is considerably lighter and more comfortable than a traditional helmet. Two additional applications of this new safety technology include medical flooring especially in hospitals and nursing homes or child play areas , as well as vehicle interiors.
Testing Methods: A modification to the NOCSAE standard test apparatus has been developed and validated for impact testing of protective headwear to include measurement of both linear and angular kinematics . This apparatus consists of a twin wire fall test system equipped with a drop arm that incorporates a 50th percentile Hybrid III head and neck assembly from HumaneticsATD. The aluminum flyarm runs on Teflon sleeves through parallel braided stainless steel wires, which are attached to mounting points in the building structure and anchored into the concrete foundation. The anvil onto which the head drop systems impacts consists of a 350mm x 350mm steel based plate. Both the Riddell Revolution Speed varsity football helmet and prototype helmet were dropped from a height 2.0 meters onto a flat steel anvil, in accordance with ASTM standards, generating an impact velocity of 6.2 m/s (13.9 mph). The following slow motion videos show testing on an unhelmeted head and prototype using this apparatus
Instrumentation: A triaxial accelerometer from PCB Piezotronics (Depew, NY) and three DTS-ARS Pro 18k angular rate sensors (Diversified Technical Systems, Seal Beach, CA) affixed to a triaxial block were installed at the center of mass of the Hybrid III head form (HumaneticsATD, Plymouth, MI). Data from the accelerometer and angular rate sensors were acquired using National Instruments (Austin, TX) compact DAQ hardware.
Analysis: In accordance with SAE J211, data from the analog sensors were acquired at 10,000 Hz, per channel, using LabView (National Instruments, Austin, TX), then filtered in Matlab (The Mathworks, Natick, MA) using a phaseless 4th order Butterworth filter with a cut off frequency of 1650Hz. Angular acceleration measures were derived from the angular velocity data based on a 5-point least squares quartic equation.
About Lloyd Industries, Inc.
Lloyd Industries, Inc., located in San Antonio, Florida, is a research and development company focused on the biomechanics of brain injuries. The company was founded in 2004 by John D. Lloyd Bio, Ph.D., CPE, CBIS, Board Certified Ergonomist and Certified Brain Injury Specialist. He has also provided expert witness services nationwide for over 20 years in the fields of biomechanics, ergonomics and human factors, specializing in the biomechanics of brain injury, including sport and motorcycle helmet cases, slips and falls, motor vehicle accidents and pediatric head trauma. Lloyd Industries is open to licensing with manufacturers to bring this much-needed technology to market for the protection of sports participants and athletes of all ages. For additional information call 813-624-8986.
Researchers Discover Objective Indicator of Concussion
Lends to opportunity to Protect Professional and Youth Sports Players from Traumatic Brain Injuries
Sport concussion researchers teamed up with football players at a Florida high school. Ten players were equipped with Riddell Revolution Speed helmets, with the embedded Simbex HITS encoders, which were worn throughout the 2011/2 football season. The HITS system recorded the severity and location of all head impacts during both football practice sessions and games.
To measure the physiological effects of acute and cumulative head impacts, players agreed to wear a wireless EEG system, which was housed on the back of the shoulder pads. In addition, heart rate variability, respiration rate as well as linear and angular motion was recorded using a Tricorder developed by ReThink Medical.
During the 2011/2- football season, several concussive level impacts were recorded. Two players were removed from the field due to suspected sport concussion / mTBI, one of whom was wearing the complete data acquisition system, including HITS encoders, Nicolet EEG and ReThink Tricorder at the time of impact and for approximately 30 minutes post-impact. For the first time we have the opportunity to investigate physiological responses and brain activity changes in response to a concussive level head impact.
Analysis of one player’s self-reported concussive impact clearly shows decreased Gamma band activity and increased Theta band activity in the frontal cortex of the brain immediately following significant head impact. This suggests that the player had reduced cognitive performance and was perhaps in a ‘drowsy’ state for about 10 minutes following impact. During this time, the player may have been dazed and confused and certainly less effective on the field. But more importantly, his ability to protect himself from a second, potentially harmful impact was greatly compromised.
The findings of our study clearly indicate compromised brain activity as a result of head impact, which appears to be correlated with the magnitude of the impact.
Normalized Power Trend Analysis. Normalized Theta (Left) and Gamma (Right) Power (log of % power within band) of a football player, who experienced a concussion following a moderately forceful head impact (Red line), show phasic modulations in power throughout the practice. Fluctuations in power rarely exceed 25% of the total average power for the recording session in Theta and Gamma frequencies. Yet, immediately following a violent hit (Red line), gamma power begins to decline rapidly and exceeds an arbitrary criterion of ±50% change from average power (peaking at 90 min.). Indeed gamma power remained within 20% of the mean for most of the duration of practice, exceeding this degree of change for over 10 minutes after the impact and two other brief episodes (around 20 min. and 50 min. for less than five minutes; Note, the first and last five minutes were ignored due to the temporal filtering artifact at both edges). Whereas, a peak in theta power coincided with the greatest change in gamma power, the degree of change from the mean normalized power never exceeded 10%. This preliminary data suggests that our algorithms provide (1) the sensitivity to detect significant change in brain activity following a concussive event, and (2) specificity in detecting which frequency band (i.e., gamma) provides the most meaningful brain signal for detecting concussion / brain trauma
Our future goals for the upcoming football season include a new micro-EEG recorder, which is in development, that will allow unobtrusive measurement of several players simultaneously during both football practice and games.
Ultimately, it is our hope that this technology will be widely available to both professional and youth teams so that medical staff can monitor the brain health of players in real-time so that injured participants can be objectively identified, effectively protected and successfully treated.
I employ state-of-the-science biomechanics resources in my evaluations, as depicted in the following figure. This biomechanics laboratory includes various certified biofidelic mannequins, dedicated test apparatus, data acquisition hardware, software and calibrated sensor instrumentation, professional photography and high speed and videography equipment.
Much of my research and work for civil law suits focusses on biomechanical evaluation of helmets, in particular sports helmets, including football and ski helmets.
For helmet testing, we have a standard NOCSAE (National Operating Committee for Standards in Athletic Equipment) head drop system
However, the standard NOCSAE system only measures forces associated with linear acceleration, which are attributed with focal head injuries, such as skull fractures. This system has a rigid neck and therefore cannot measure rotational or angular accelerations, which are associated with traumatic brain injuries, such as concussion and subdural hematomas. We have a modified helmet drop test system, developed in collaboration with the University of Maine, Advanced Manufacturing Center, validation of which has been published in a peer-reviewed journal.
The following image shows both the NOCSAE and modified helmet test systems in parallel.
Recent research shows that standard linear impact tests may not fully account for impact forces as they do not incorporate angular velocity. Therefore, I have created an inverted pendulum system, which is more representative of a standing fall
Additionally, the biomechanics laboratory is equipped with the following resources:
Monorail head drop assembly
Twin wire guided drop system (NOCSAE)
Weighted pendulum impactor
Linear bearing table
Height-adjustable, eletromagenetically-controlled freefall drop platform
20,000N impact force plate
880lb ceiling mounted lift system
Certified biofidelic adult headforms
CRABI12 biofidelic infant mannequin
Hybrid III 3-yr old biofidelic mannequin (KSS)
National Instruments 32 channel USB-6343 X-series data acquisition system
LabView 2009 data acquisition software.
Calibrated sensors, including Kistler and PCB Piezotronics tri-axial accelerometers, MEMS triple axis digital gyroscopes, and PCB Piezotronics uni-axial and tri-axial load cells.
Selection of flooring materials, including carpeting, wood and laminates as well as concrete and wood sub-flooring surrogates
Professional still photography equipment
Normal speed and high speed (up to 1kHz) videography equipment
Dr. Lloyd’s unique capability as a helmet expert is in the biomechanical evaluation of helmets, specifically, football, sports and motorcycle helmets. Helmets are designed to reduce the risk of blunt force trauma to the head, however protection against diffuse traumatic brain injury is often inadequate. Dr. Lloyd is often called upon to opine whether the head and brain injuries may or may not have been prevented by head protection.
Using this apparatus, helmet expert Dr. Lloyd and neurologist Dr. Frank Conidi of the Florida Center for Headache and Sports Neurology have presented a series of studies at the American Academy of Neurology meetings. Their work was publicized by the AAN in a press-release titled “How Well Do Football Helmets Protect Players from Concussions“. Dr. Lloyd and Dr. Conidi published a scientific article in the Journal of Neurosurgery titled “Brain Injury in Sports“. This article documents the limited protection against traumatic brain injuries afforded by many current varsity football helmets.
Example Motorcycle Helmet Expert Case
Dr. Lloyd provided biomechanical analysis on a recent motorcycle accident case in which an automobile crossed the path of an unhelmeted rider traveling at approximately 25 miles per hour. The motorcyclist’s head shattered the driver’s side window, leading to catastrophic brain injury
Dr. Lloyd was asked to opine as to whether or not a motorcycle helmet would have prevented these injuries. A test apparatus was constructed using an exemplar automobile driver’s door and window to measure the forces acting on a crash test dummy head.
The following high speed videos and data were captured showing the helmeted versus unhelmeted conditions.
We learned that, had the motorcyclist been wearing a helmet during the subject collision, he would have most likely sustained fatal neck injuries as the helmet was deflected by the window, producing unsurvivable neck extension, as shown below:
Test results and video documentation were presented at deposition and proved highly valuable.
Please call Dr. Lloyd at 813-624-8986 or email DrJohnLloyd@Tampabay.RR.com to discuss how he can be of help to you with your case.
How Well Do Football Helmet Protect Against Concussion and Brain Injury?
Football helmet research presented by John Lloyd, PhD – BRAINS, Inc. & Frank Conidi, MD – Florida Center for Headache and Sports Neurology at the 66th Annual Meeting of the American Academy of Neurology, 2014
Sports related concussion is the most widely publicized neurological disorder, with football accounting for the highest incidence across all sports. There is a silent epidemic of these invisible injuries across players of all ages from youth through professional, resulting in a 3-fold increase in ER visits among high school players from 2000-2010. It is estimated that a quarter of a million of these injuries each year have long-term consequences. A single moderate to severe brain injury can leave one at risk for early onset dementia, while repeated mild concussions may have the same effects (Giza).
The football helmet became mandatory in the 1930’s to provide protection against catastrophic head injuries. Over the past eighty years there have been significant modifications in football helmet design. Yet despite advances in technology there is still little evidence that helmets offer significant protection against concussion and traumatic brain injury (Giza). hile the widely utilized Simbex HITS system and the Virginia Tech STAR rating system attempt to measure helmet performance, neither offer a direct measure of concussion or brain injury risk.
Methods
According to Holbourn, risk of focal head injury, such as skull fracture and brain contusion, can be expressed in terms of linear acceleration, while the risk of concussion, axonal injury and diffuse brain injury is associated with angular/rotational acceleration. The standard NOCSAE / ASTM helmet tests only measure forces associated with linear acceleration and therefore fail to account for risk of brain injury.
A modified test apparatus, incorporating a Hybrid III crash test dummy head and neck, has been validated by Caccese and Lloyd. This method induces a rotational inertia on impact, thereby facilitating measurement of risk of focal head and diffuse brain injuries.
We purchased 60 football helmets, including three samples each of 20 different models. All helmets were dropped five times from a height of 2.0 meters onto a steel plate, generating an impact velocity of 13.9 mph.
Football Helmet Results
Our findings show that football helmets vary widely in terms of their performance to protect against focal head injury and concussion / diffuse brain injury. All tested football helmets, including the 1930s leatherhead meet the minimum performance criteria of 275G as set by the ASTM F717 standard. However, this standard does not account for duration of impact, which is a critical factor. Moreover, ASTM F717 does nothing to set helmets performance standards in terms of protection against concussion and brain injury.
By design, helmets reduce impact force by increasing the impact duration. But, as demonstrated by Depreitere (blue) and Lowenhielm (red) increasing impact duration actually lowers the brain injury threshold. Head injury risk was calculated with respect to the140g threshold for 7msec impact documented by Ono, wwhile brain injury risk was calculated based on Ommaya’s1700 rad/s^2 tolerance limit for moderate AIS2 brain injury, which concurs with Rowan and Duma’s top 25% of sub-concussive impacts.
Results are presented below, where % reduction of head injury risk is shown in red and % reduction of concussion/mTBI is presented in blue.
Bars above the x-axis indicate that the helmet performs better than the documented threshold, while those below the x-axis did not meet our performance thresholds.
It is noted, interestingly, that the 1930s Goldsmith leatherhead helmet actually outperformed several contemporary football helmets in terms of protecting against concussion and brain injury, including the Adams a2000 Pro, the Rawlings Quantum and the Riddell 360.
Based on our research, the top 3 varsity helmets are: Xenith X1, Schutt Air XP Pro, and Rawlings Quantum Plus, respectively. The top 10 helmets are presented below, based on their protection against traumatic focal head injuries and diffuse brain injuries:
Conclusions
None of the football helmets on the market today offer what most would consider adequate protection against concussions and traumatic brain injuries. A shift in thinking towards lighter high-tech materials for helmets, teaching proper hitting and tackling techniques, pre and in-season isometric and isokinetic cervical strengthening programs, and continued concussion awareness and education are the best means of protecting athletes of all levels from the consequences of concussion and traumatic brain injury.
Future Research
It is hypothesized that oblique impacts present even longer impact durations, which may explain why such seemingly innocuous impacts cause increased incidence of concussion.
Embracing the findings from testing of the 1930s Goldsmith leatherhead, a new generation of soft football helmets is proposed, utilizing today’s advanced non-Newtonian materials, which we anticipate might outperform contemporary helmets in terms of protection against both traumatic head and brain injuries.

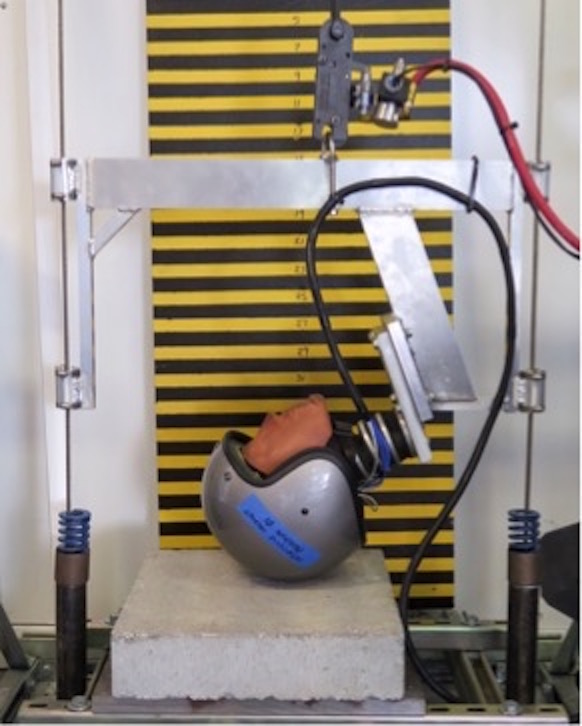



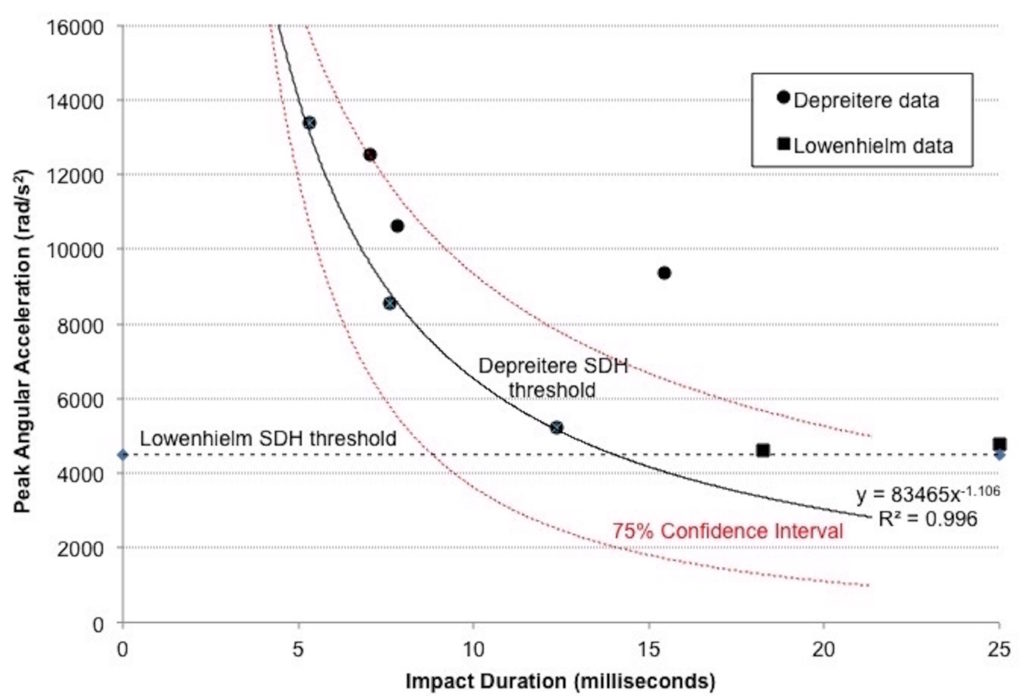 Helmets decrease peak translational force by extending the impulse duration. In the case of motorcycle helmets, typical impulse duration is approximately 12 milliseconds. With reference to Figure 1, above, this suggests that bridging vein rupture may result with peak angular accelerations in the order of 5,000 rad/s2, but may be as low as 3,000 rad/s2 after adjusting for standard error of the mean in this limited dataset.
Helmets decrease peak translational force by extending the impulse duration. In the case of motorcycle helmets, typical impulse duration is approximately 12 milliseconds. With reference to Figure 1, above, this suggests that bridging vein rupture may result with peak angular accelerations in the order of 5,000 rad/s2, but may be as low as 3,000 rad/s2 after adjusting for standard error of the mean in this limited dataset.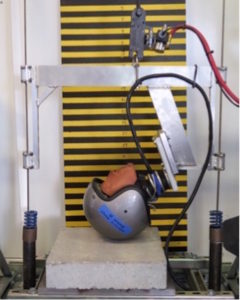

 Five samples of each motorcycle helmet model were purchased in new condition. Each helmet was impacted one time in the frontal and/or occipital region at an impact velocity of approximately 8.3 meters per second (18.5 mph), which was verified computationally. Repeatability of the tests was confirmed at the start and end of data collection by dropping the Hybrid III headform from a height of 2.0 m onto a Modular Elastomer Programmer (MEP) pad of 25 mm thickness and durometer 60A. Standard Error of the Mean of 0.061 was computed based on peak angular accelerations for pre and post MEP pad drop tests.
Five samples of each motorcycle helmet model were purchased in new condition. Each helmet was impacted one time in the frontal and/or occipital region at an impact velocity of approximately 8.3 meters per second (18.5 mph), which was verified computationally. Repeatability of the tests was confirmed at the start and end of data collection by dropping the Hybrid III headform from a height of 2.0 m onto a Modular Elastomer Programmer (MEP) pad of 25 mm thickness and durometer 60A. Standard Error of the Mean of 0.061 was computed based on peak angular accelerations for pre and post MEP pad drop tests.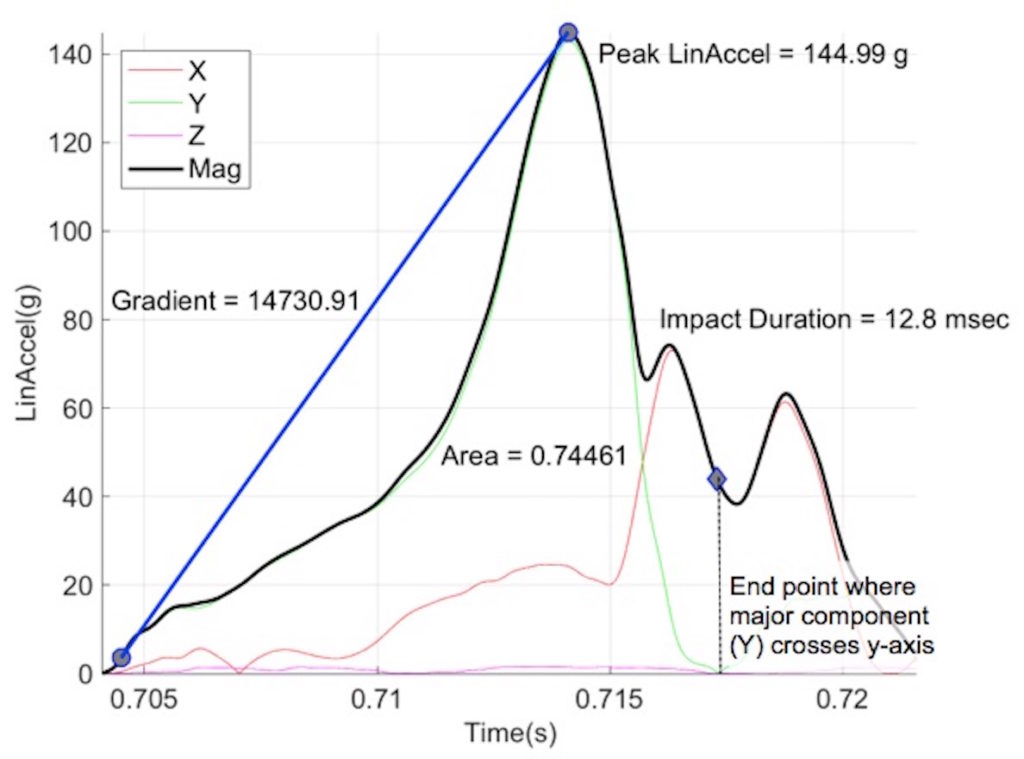 An analysis method validated by Takhounts
An analysis method validated by Takhounts 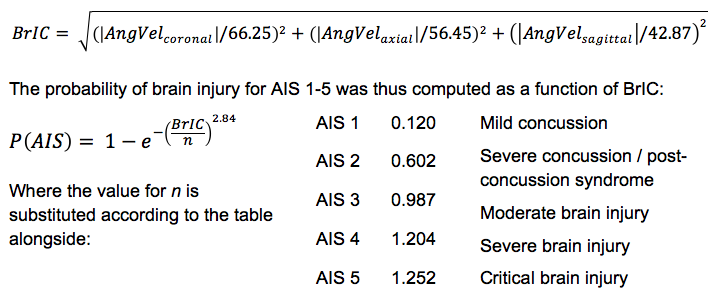
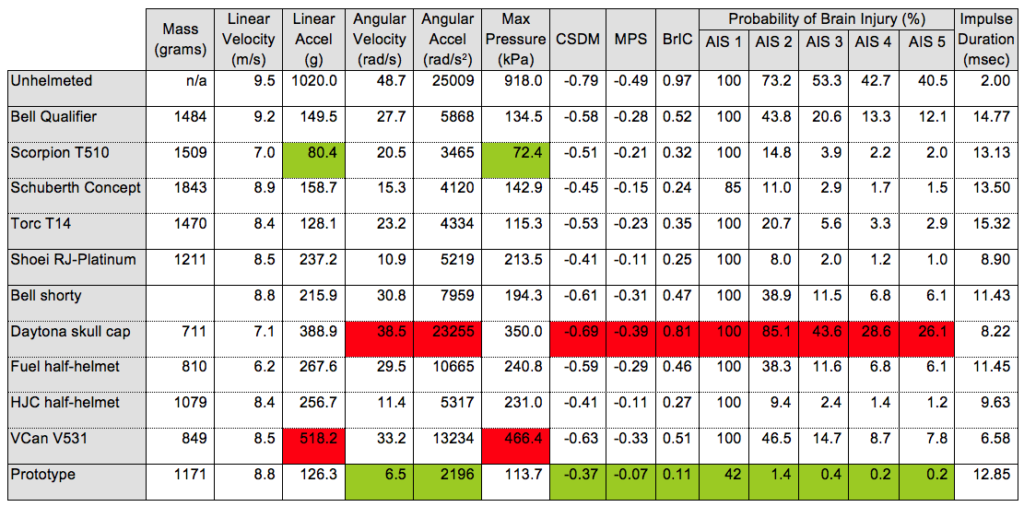
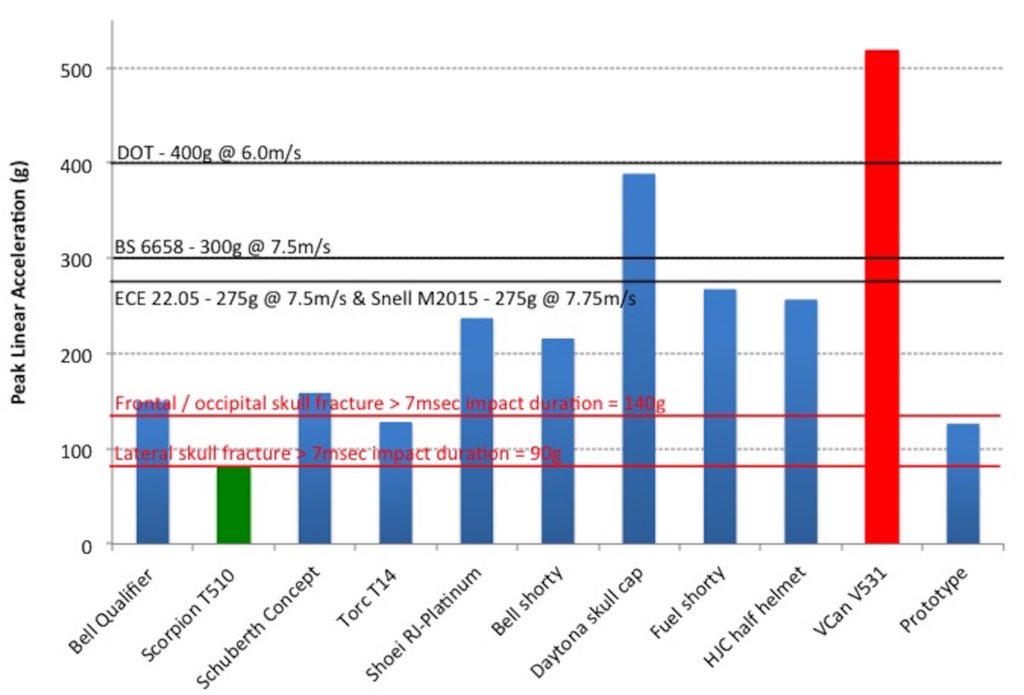
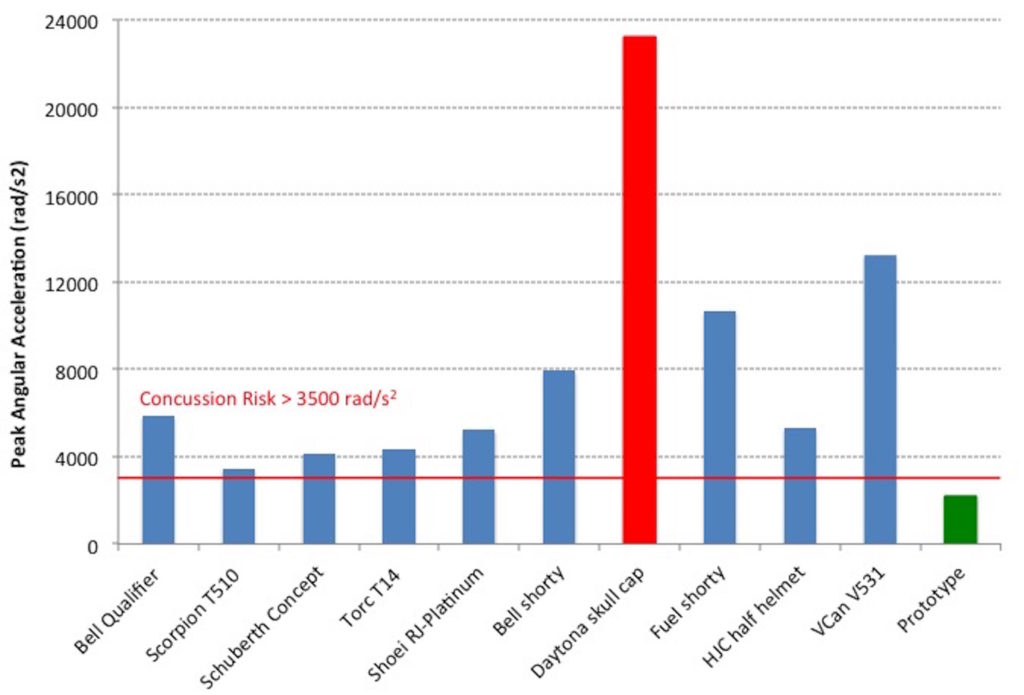
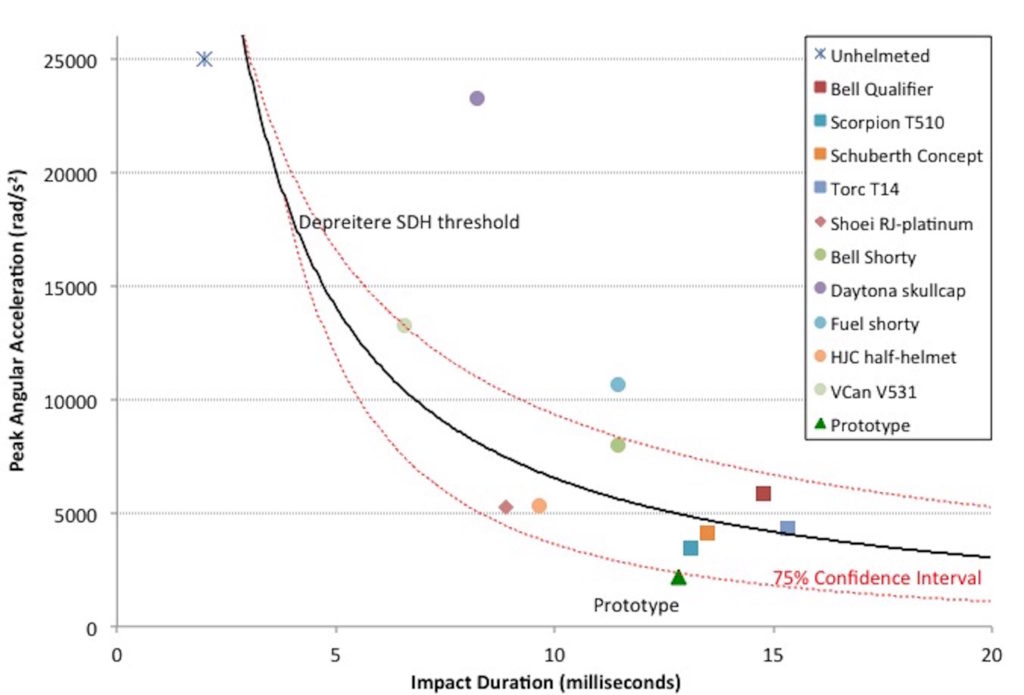
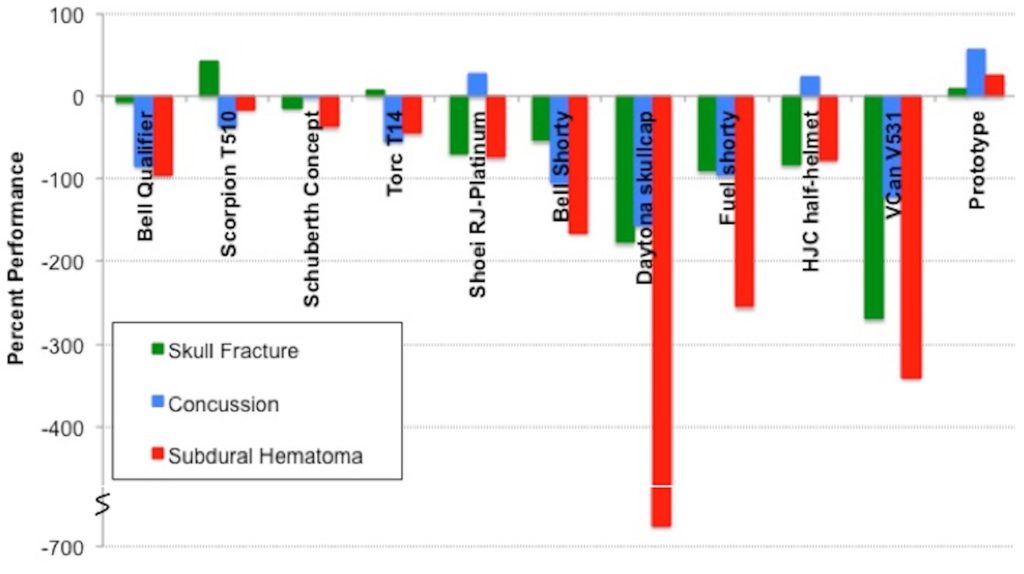
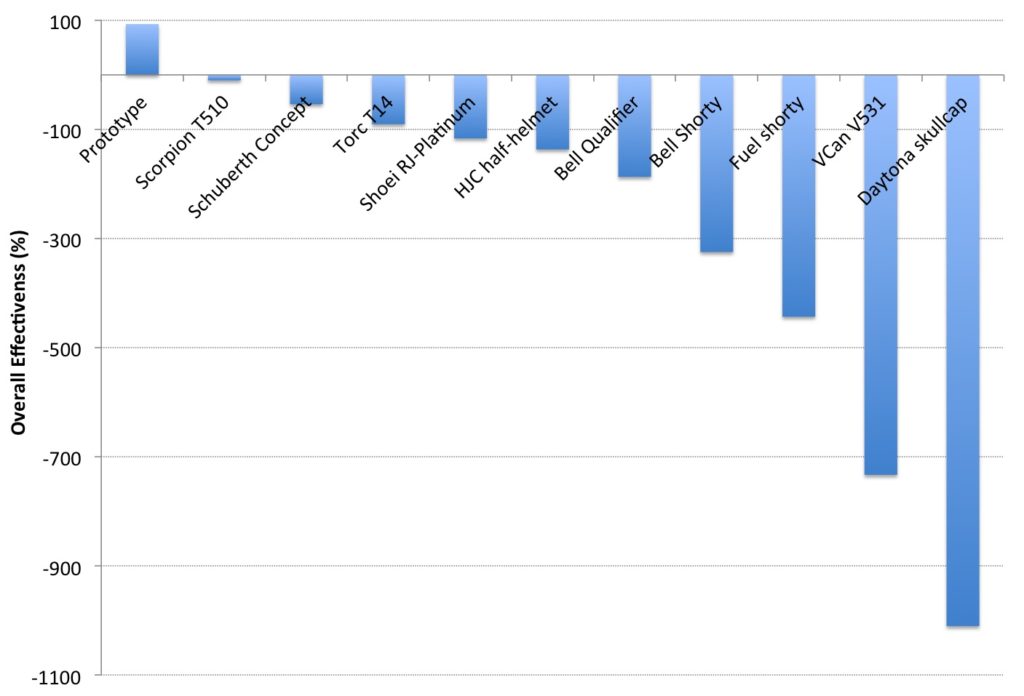

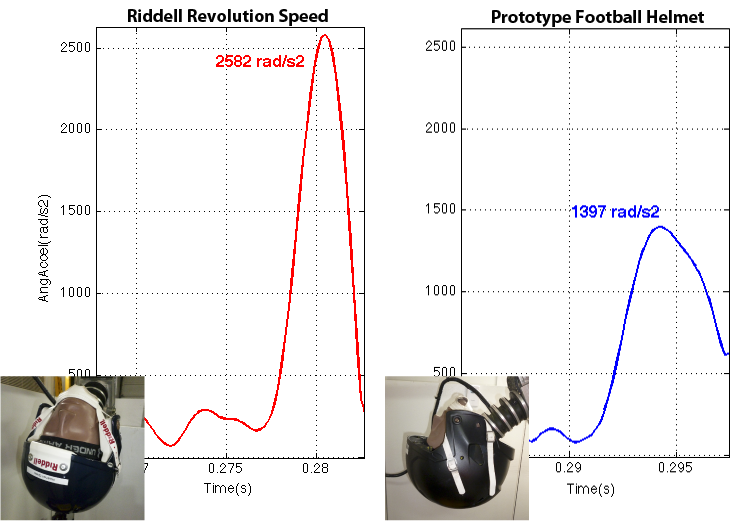





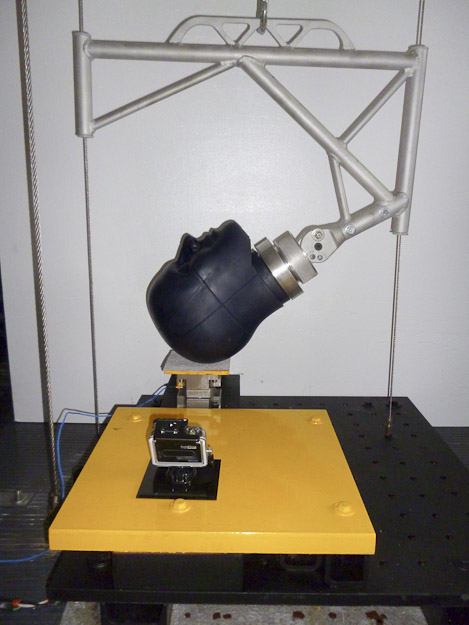
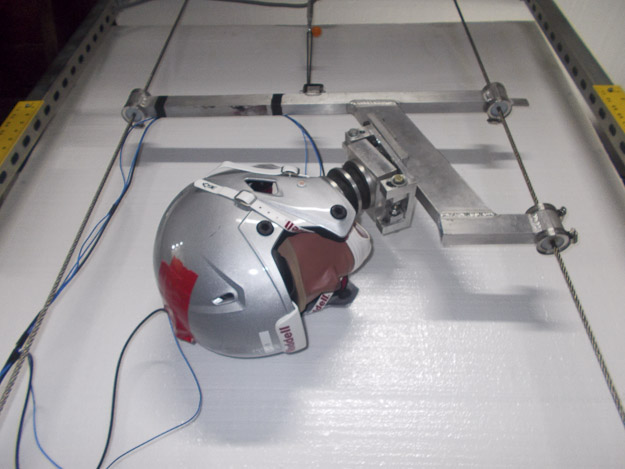
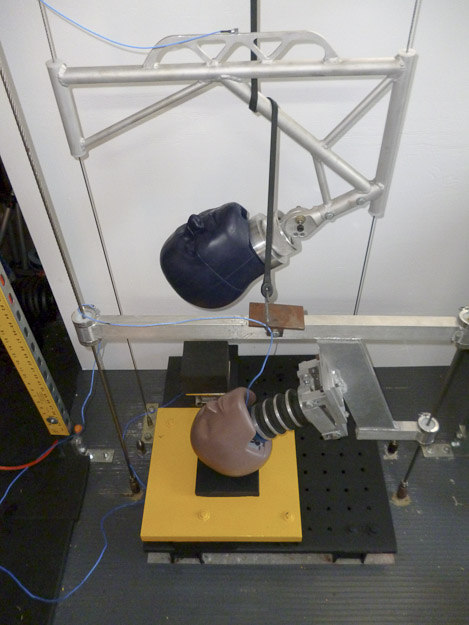






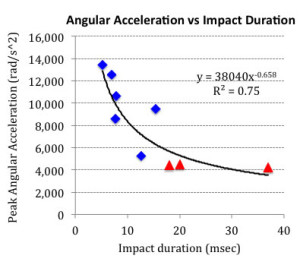 By design, helmets reduce impact force by increasing the impact duration. But, as demonstrated by
By design, helmets reduce impact force by increasing the impact duration. But, as demonstrated by