Researchers Discover Objective Indicator of Concussion
Lends to opportunity to Protect Professional and Youth Sports Players from Traumatic Brain Injuries
Sport concussion researchers teamed up with football players at a Florida high school. Ten players were equipped with Riddell Revolution Speed helmets, with the embedded Simbex HITS encoders, which were worn throughout the 2011/2 football season. The HITS system recorded the severity and location of all head impacts during both football practice sessions and games.
To measure the physiological effects of acute and cumulative head impacts, players agreed to wear a wireless EEG system, which was housed on the back of the shoulder pads. In addition, heart rate variability, respiration rate as well as linear and angular motion was recorded using a Tricorder developed by ReThink Medical.
During the 2011/2- football season, several concussive level impacts were recorded. Two players were removed from the field due to suspected sport concussion / mTBI, one of whom was wearing the complete data acquisition system, including HITS encoders, Nicolet EEG and ReThink Tricorder at the time of impact and for approximately 30 minutes post-impact. For the first time we have the opportunity to investigate physiological responses and brain activity changes in response to a concussive level head impact.
Analysis of one player’s self-reported concussive impact clearly shows decreased Gamma band activity and increased Theta band activity in the frontal cortex of the brain immediately following significant head impact. This suggests that the player had reduced cognitive performance and was perhaps in a ‘drowsy’ state for about 10 minutes following impact. During this time, the player may have been dazed and confused and certainly less effective on the field. But more importantly, his ability to protect himself from a second, potentially harmful impact was greatly compromised.
The findings of our study clearly indicate compromised brain activity as a result of head impact, which appears to be correlated with the magnitude of the impact.
Normalized Power Trend Analysis. Normalized Theta (Left) and Gamma (Right) Power (log of % power within band) of a football player, who experienced a concussion following a moderately forceful head impact (Red line), show phasic modulations in power throughout the practice. Fluctuations in power rarely exceed 25% of the total average power for the recording session in Theta and Gamma frequencies. Yet, immediately following a violent hit (Red line), gamma power begins to decline rapidly and exceeds an arbitrary criterion of ±50% change from average power (peaking at 90 min.). Indeed gamma power remained within 20% of the mean for most of the duration of practice, exceeding this degree of change for over 10 minutes after the impact and two other brief episodes (around 20 min. and 50 min. for less than five minutes; Note, the first and last five minutes were ignored due to the temporal filtering artifact at both edges). Whereas, a peak in theta power coincided with the greatest change in gamma power, the degree of change from the mean normalized power never exceeded 10%. This preliminary data suggests that our algorithms provide (1) the sensitivity to detect significant change in brain activity following a concussive event, and (2) specificity in detecting which frequency band (i.e., gamma) provides the most meaningful brain signal for detecting concussion / brain trauma
Our future goals for the upcoming football season include a new micro-EEG recorder, which is in development, that will allow unobtrusive measurement of several players simultaneously during both football practice and games.
Ultimately, it is our hope that this technology will be widely available to both professional and youth teams so that medical staff can monitor the brain health of players in real-time so that injured participants can be objectively identified, effectively protected and successfully treated.
The following is a case study in which biomechanics expert, Dr. John Lloyd, evaluated the risk of concussion and brain injury associated with headrest impact in rear end crashes.
Headrest Impact Test Apparatus:
In accordance with prior published test methods[1],[2],[3], a test apparatus was constructed to evaluate the biomechanical protection afforded by an exemplar automobile headrest against head and brain injuries during occipital head impacts in a simulated rear-end motor vehicle collision.
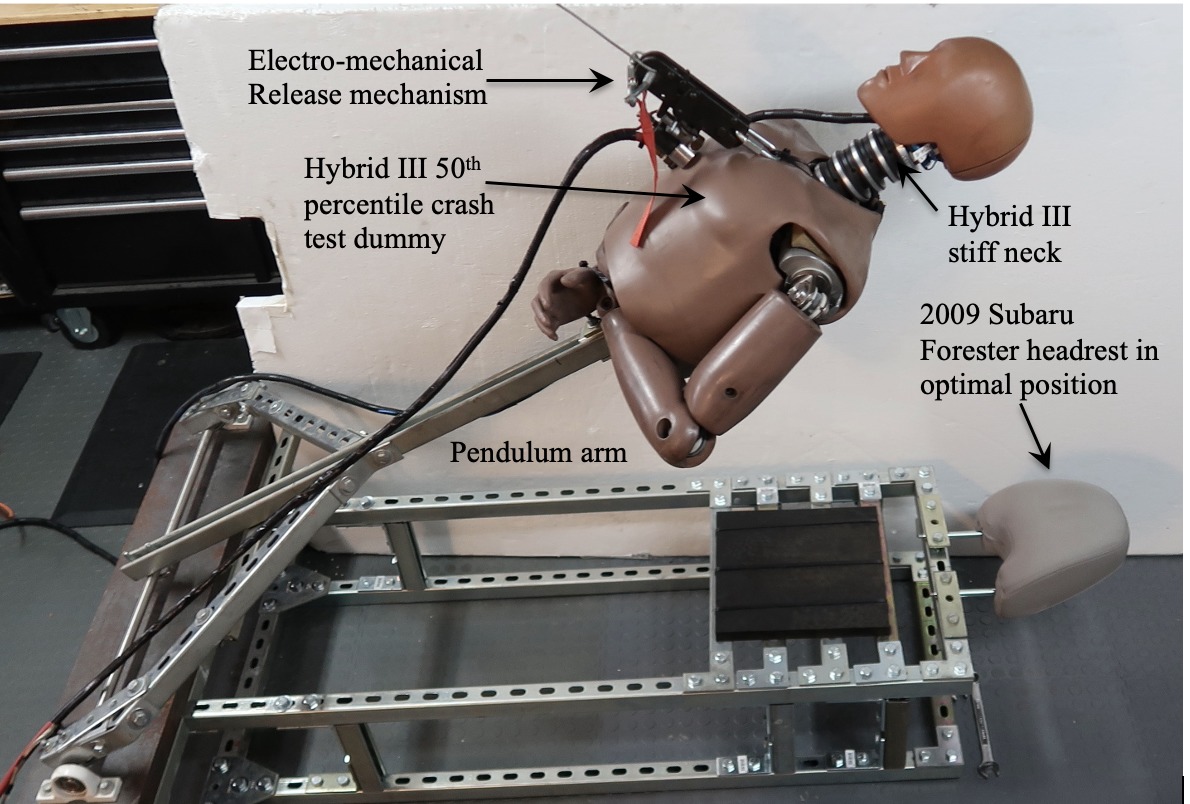
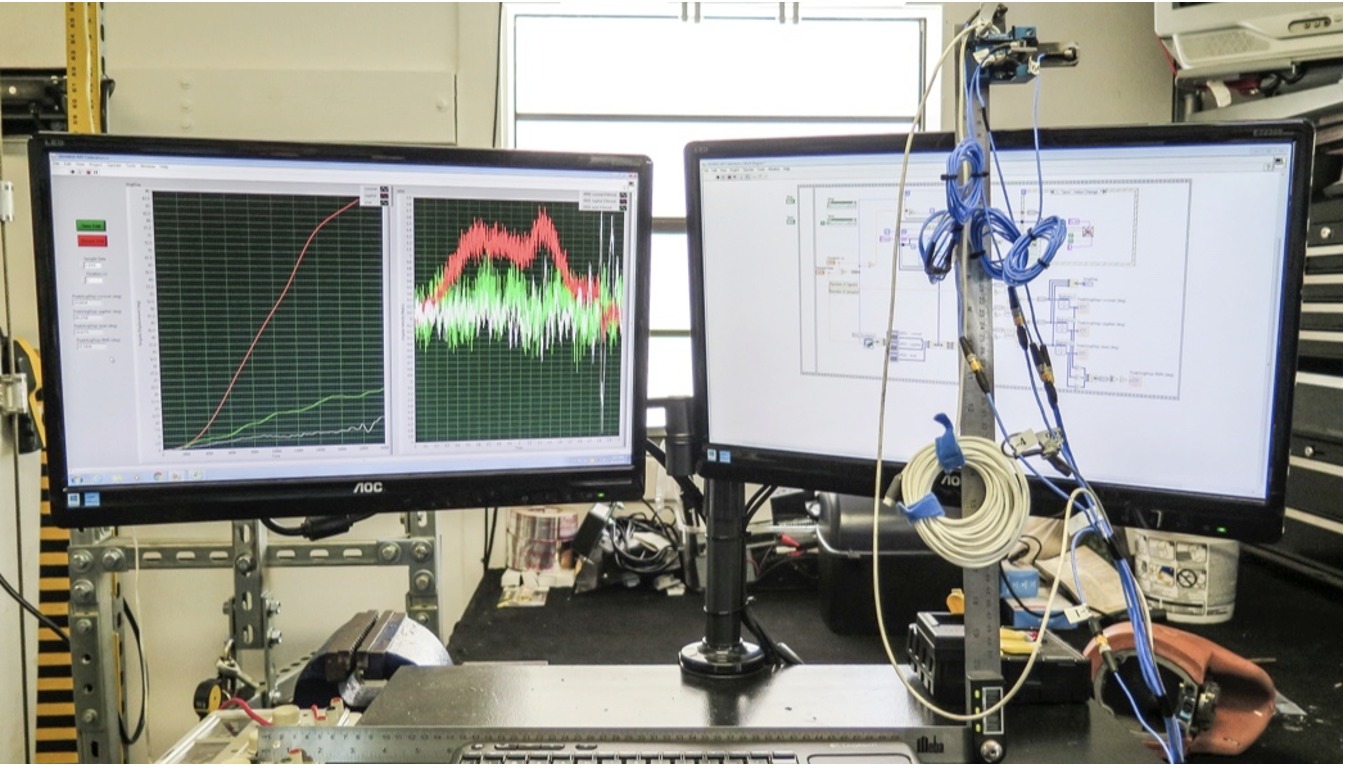
The apparatus involves a pendulum arm, attached by bearing housings to a weighted base. The upper body, including neck and head of a 50th percentile Hybrid III crash test dummy was mounted to the pendulum arm. Data acquisition was initiated by triggering an electromechanical release mechanism, allowing the mannequin to fall, under acceleration due to gravity, until the crash test dummy impacted the headrest and backrest (Figure 1).
Figure 1: Test apparatus
The fundamental elements and principles of this testing have been utilized in other laboratories. By utilizing a Hybrid III neck, the head impact tests are more realistic, causing head rotation at the axis between the head and neck, which produces measures of head and brain angular kinematics. The methods presented herein are based upon standardized test methodologies and published research.
Instrumentation
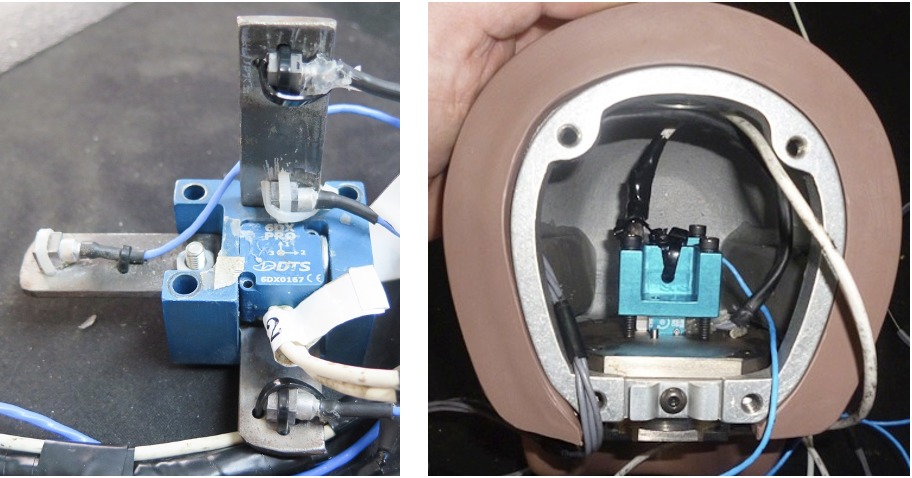
Four PCB Piezotronics tri-axial accelerometers (model # 356A01) were mounted in an X,Y,Z array at the center of mass of the Hybrid III headform, along with a tri-axial angular rate sensor produced by Diversified Technical Systems (composite Figure 2).
Figure 2: Sensor installation in Hybrid III headform
Sensor Calibration:
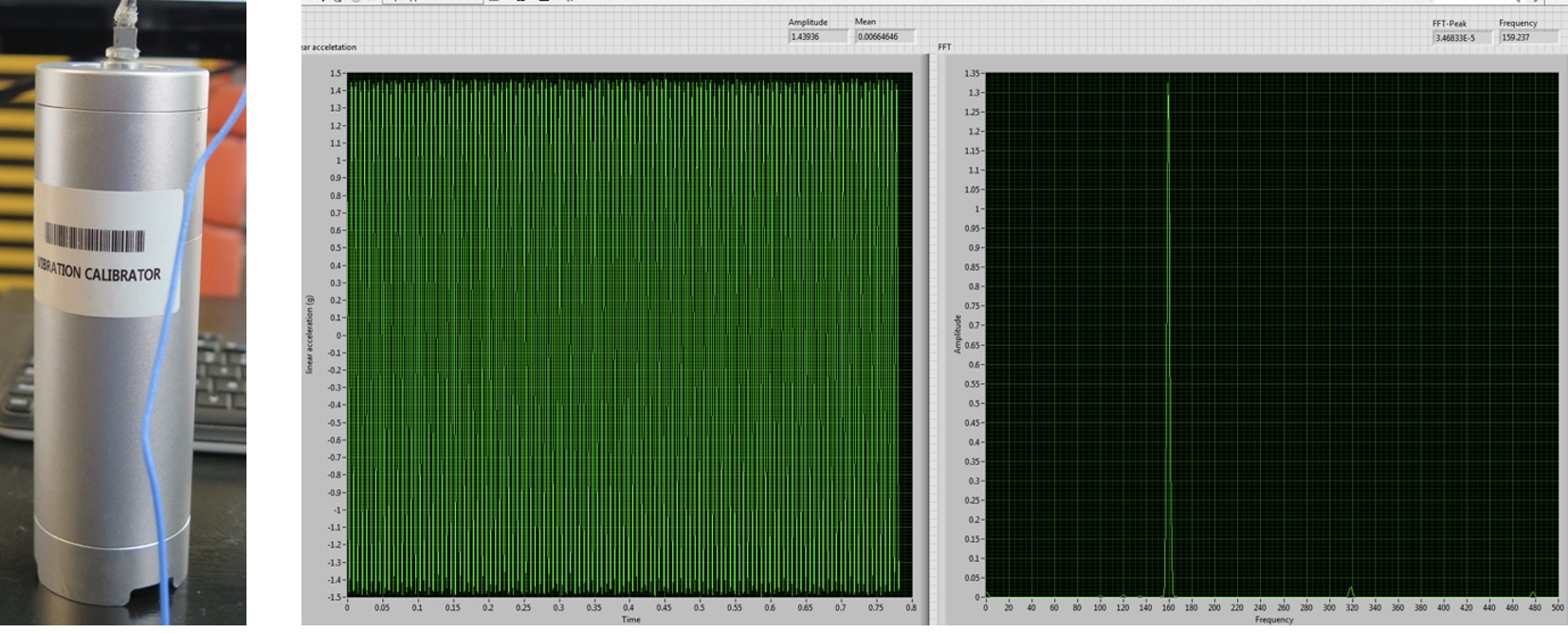
All sensors were calibrated by the manufacturer. Verification of calibration of the linear accelerometers was performed prior to testing using a calibration shaker. Results indicate that the sensors were operating in the specified frequency range and output (Figure 3).
Figure 3: Pre-test verification of linear accelerometer sensors
For the angular rate sensor, a simple validation method was devised in which the sensor was affixed to a digital goniometer that was rotated through a 90-degree angle. Using LabVIEW software, the integral of angular rate was computed, reflecting concurrence with the digital goniometer for all three planes of motion (Figure 4).
Figure 4: Pre-test validation of angular rate sensor calibration
Headrest Impact Testing:
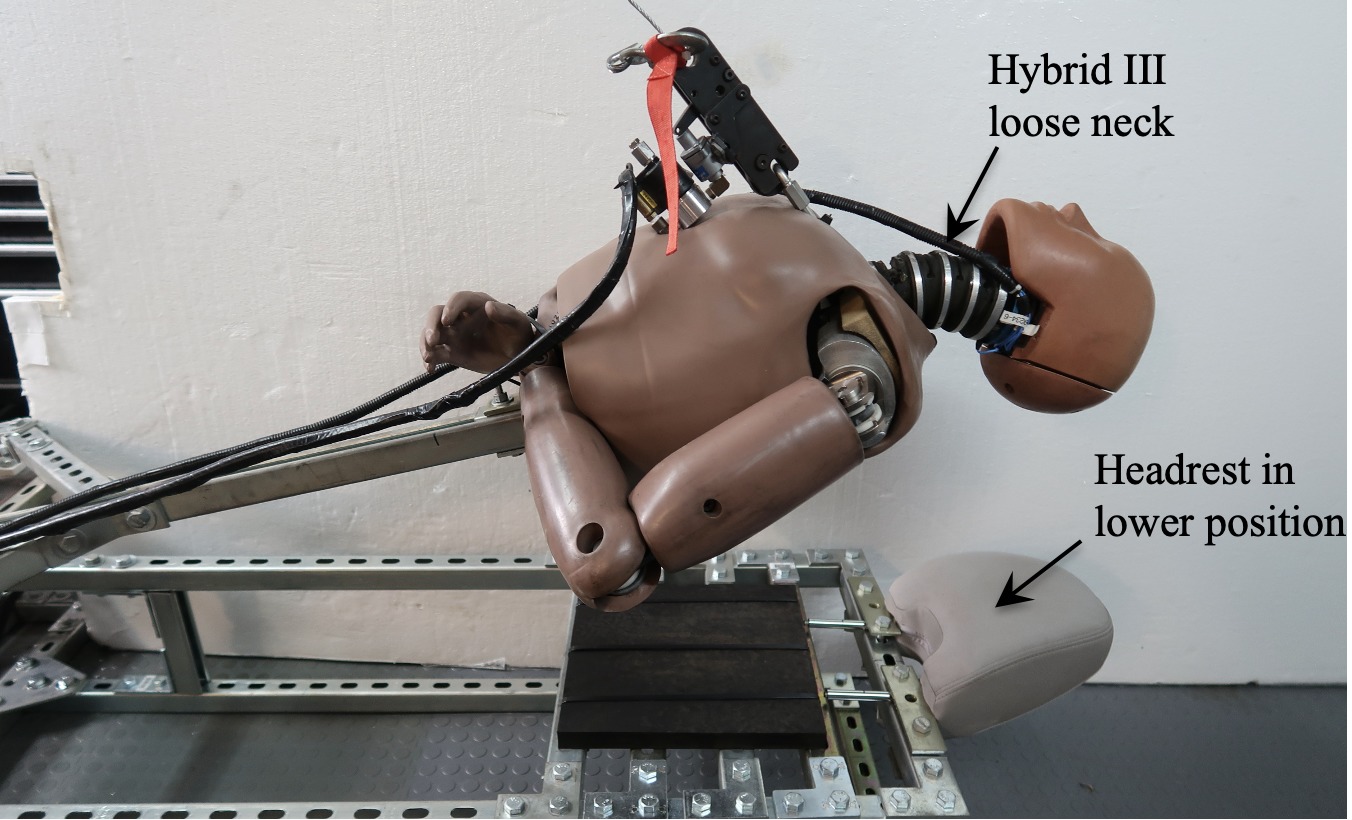
The mannequin head was raised from the headrest in 2-inch increments from 2 inches to 30 inches, generating head impact speeds from 1 to 25 miles per hour. Two headrest positions were evaluated, along with two different Hybrid III necks representative of a stiff and relaxed neck (Figure 5), for a total of sixty tests.
Figure 5: Test apparatus with Hybrid III loose neck and headrest in lower position
Data Acquisition and Analysis:
Data from the analog sensors were acquired in accordance with SAE J211 [4], using a National Instruments compact DAQ data acquisition system and LabVIEW software (National Instruments, Austin, TX). The raw data was then filtered in MATLAB (The MathWorks, Natick, MA) using a phaseless eighth-order Butterworth filter with cutoff frequencies of 1650 Hz and 300Hz for the linear accelerometers and angular rate sensors, respectively.
Angular acceleration values for sagittal, coronal and axial planes were computed from the angular velocity data using the 5-point central difference by least squares method (Equation 1):
Equation 1: Five-point central difference by least squares method
Angular acceleration vales were also derived from the array of linear accelerometers, by the mathematical method documented by Padgaonkar et al [5].
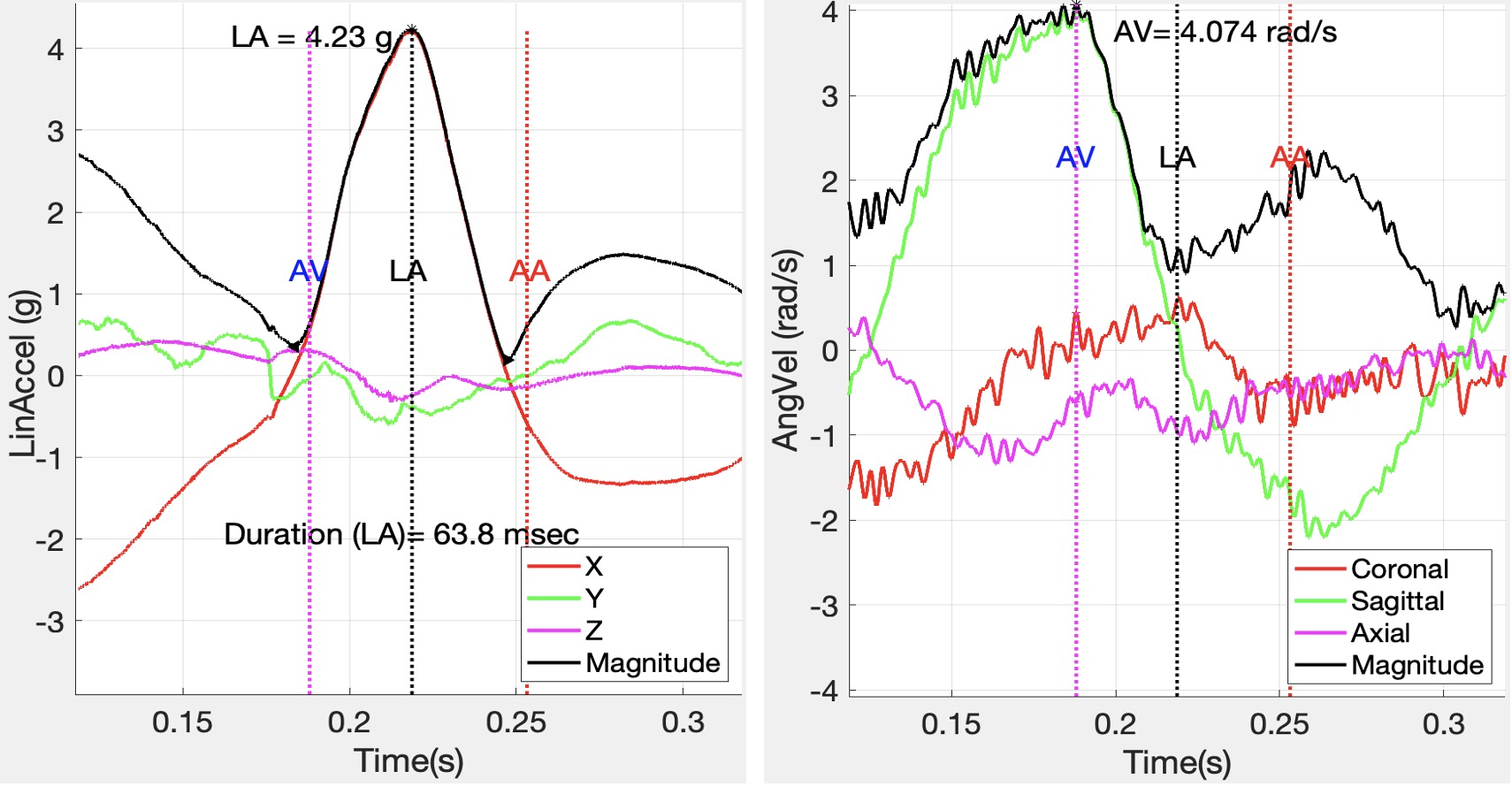
Linear velocity was calculated by integrating linear acceleration. Mathematical methods were performed using Matlab to compute characteristic values from variables of interest. Figure 6, below illustrates peak linear acceleration and angular velocity associated with a 6.8 mph occipital head impact against a headrest.
Figure 6: Linear acceleration and angular velocity associated with headrest impact
It is noted that the major component of linear acceleration was in the X-axis (anterior-posterior), while the major component of angular velocity was in the sagittal plane, as expected.
Linear acceleration values were used to calculate Maximum Pressure (Equation 2), Gadd Severity Index (GSI) (Equation 3), and Head Injury Criterion (HIC15) (Equation 4).
Equation 2: Maximum Pressure
Equation 3: Gadd Severity Index
The Head Injury Criterion (HIC) is an empirical measure of impact severity describing the relationship between the linear acceleration magnitude, duration of impact and the risk of head trauma (Equation 4).
Equation 4: Head Injury Criterion
where a is resultant head acceleration, t2-t1 < 15 msec
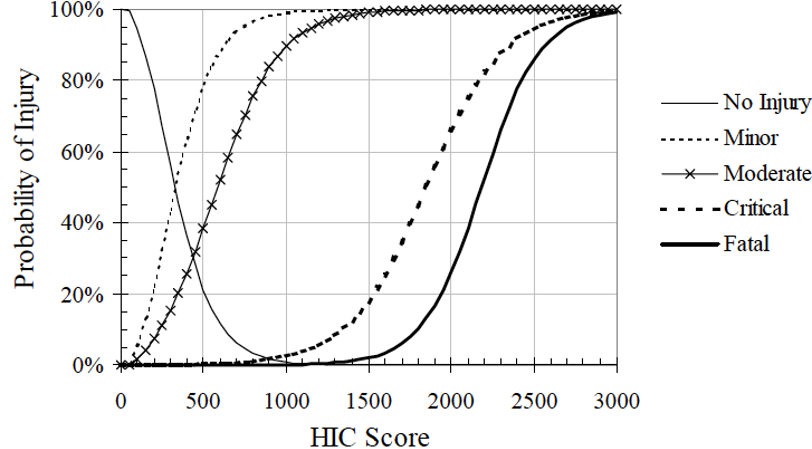
With reference to the Figure 7, below, the HIC value is used to predict the risk of head trauma: Minor –skull trauma without loss of consciousness; nose fracture; superficial injuries Moderate – skull trauma with or without dislocated skull fracture and brief loss of consciousness. Fracture of facial bones without dislocation; deep wound(s) Critical – Cerebral contusion, loss of consciousness for more than 12 hours with intracranial hemorrhaging and other neurological signs; recovery uncertain.
Figure 7: Probability of specific head trauma level based on HIC value
Peak angular velocity was determined as the maximum angular velocity related to peak linear acceleration impact time. Angular velocity values were used to derive Maximum Principal Strain (MPS) (Equation 5), Cumulative Strain Damage Measure (CSDM) (Equation 6), and Brain Rotational Injury Criterion (BrIC) (Equation 7).
Equation 5: Maximum Principal Strain
Equation 6: Cumulative Strain Damage Measure
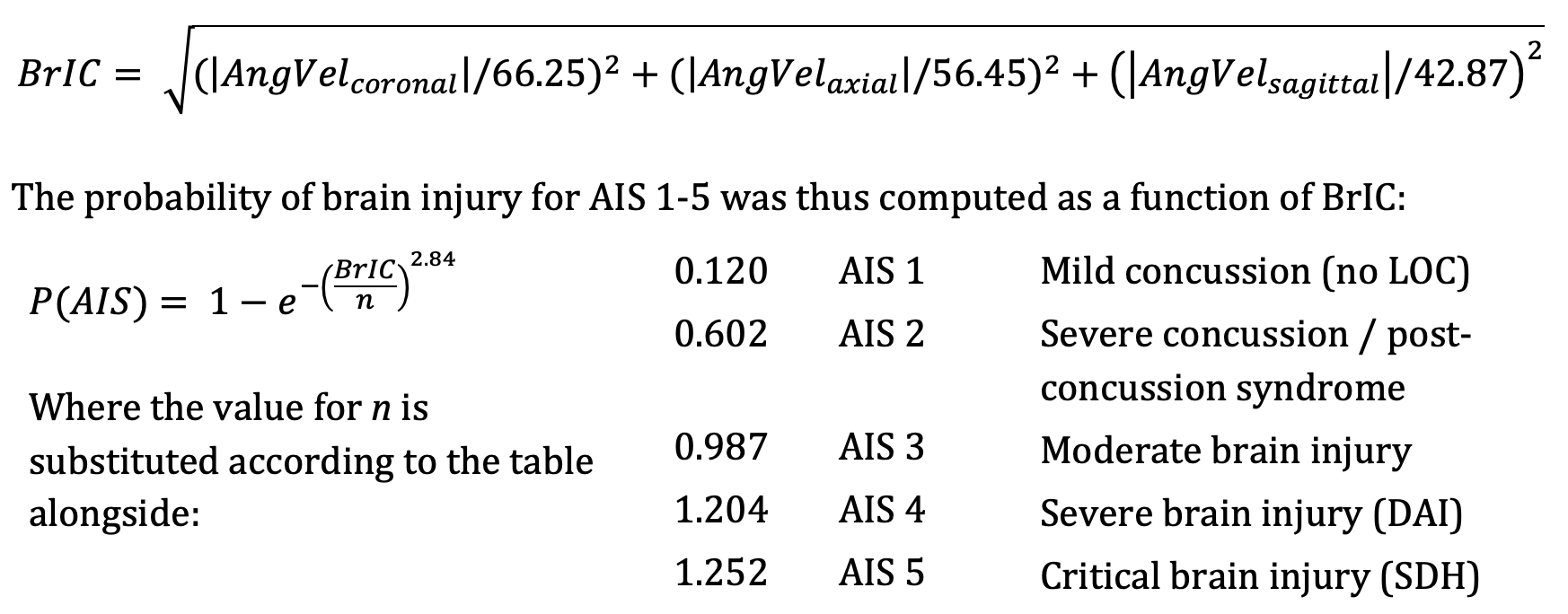
An analysis method validated by Takhounts [6] establishes physical injury criteria for various types of traumatic brain injury and uses Anthropomorphic Test Device (ATD) data to establish a kinematically based brain injury criterion (BrIC) for use with ATD impact testing. This method was utilized to express risk of diffuse brain injury according to the revised AIS scale [7] in terms of peak angular head kinematics, where:
Equation 7: Brain Rotational Injury Criterion
Headrest Impact Results:
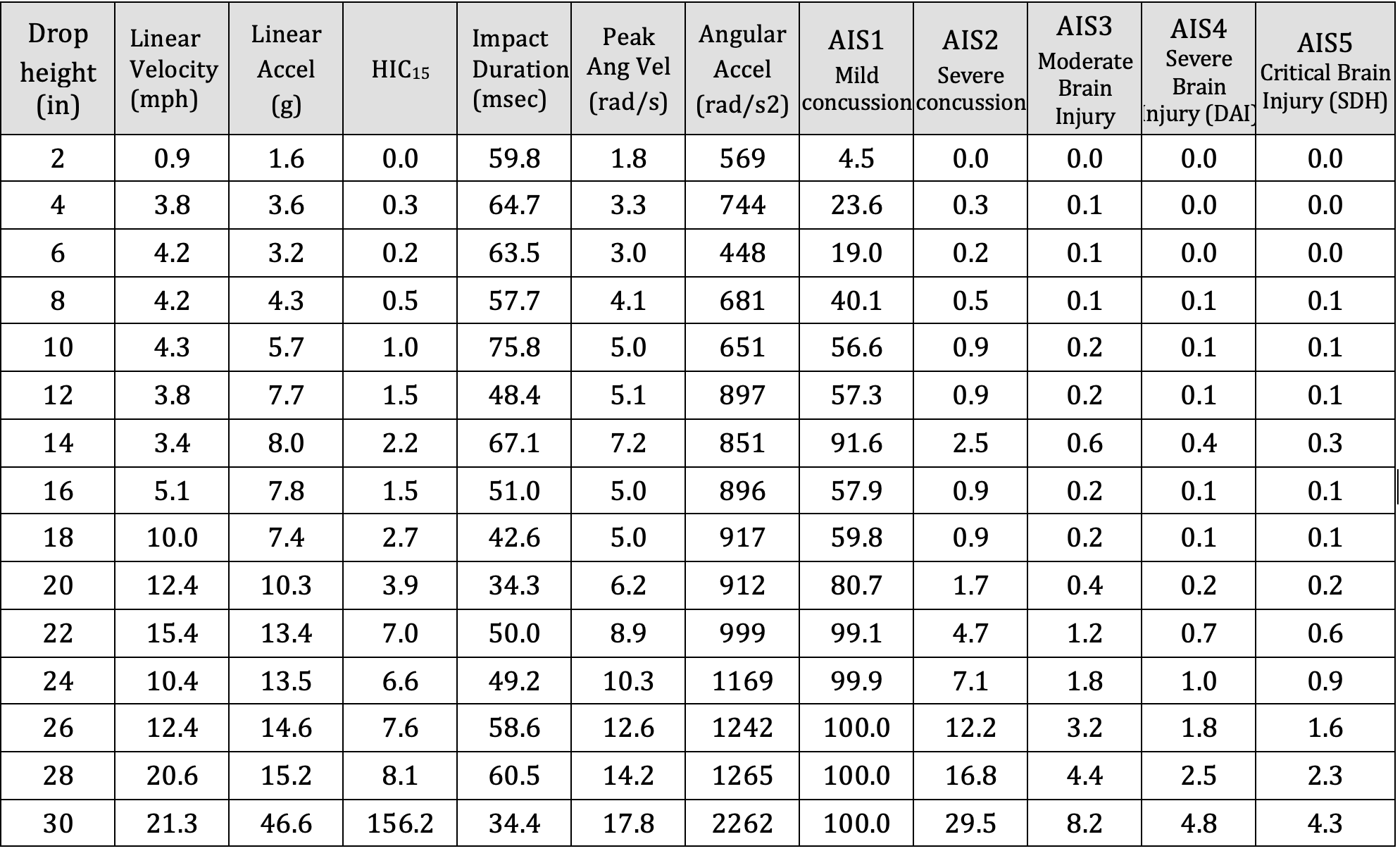
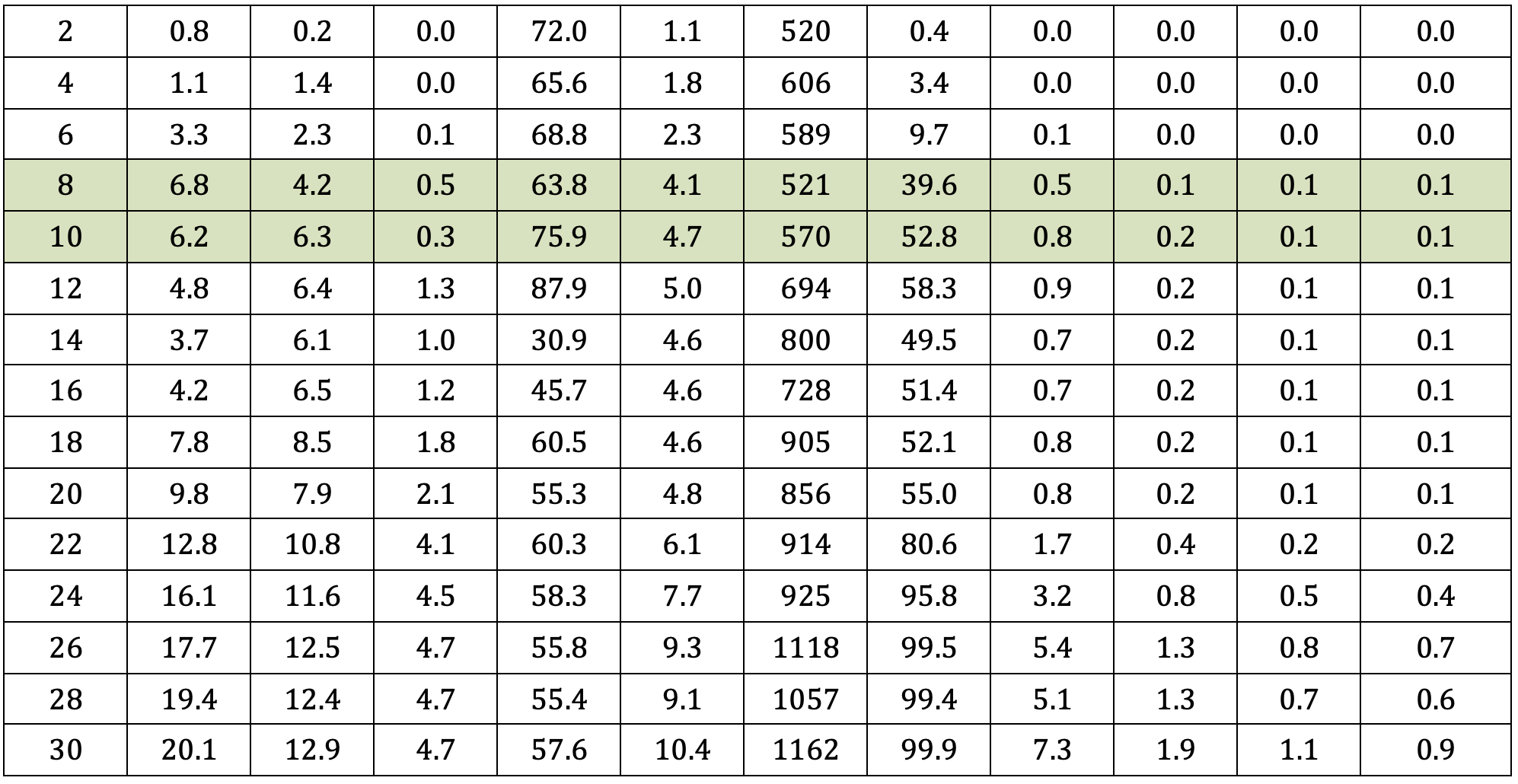
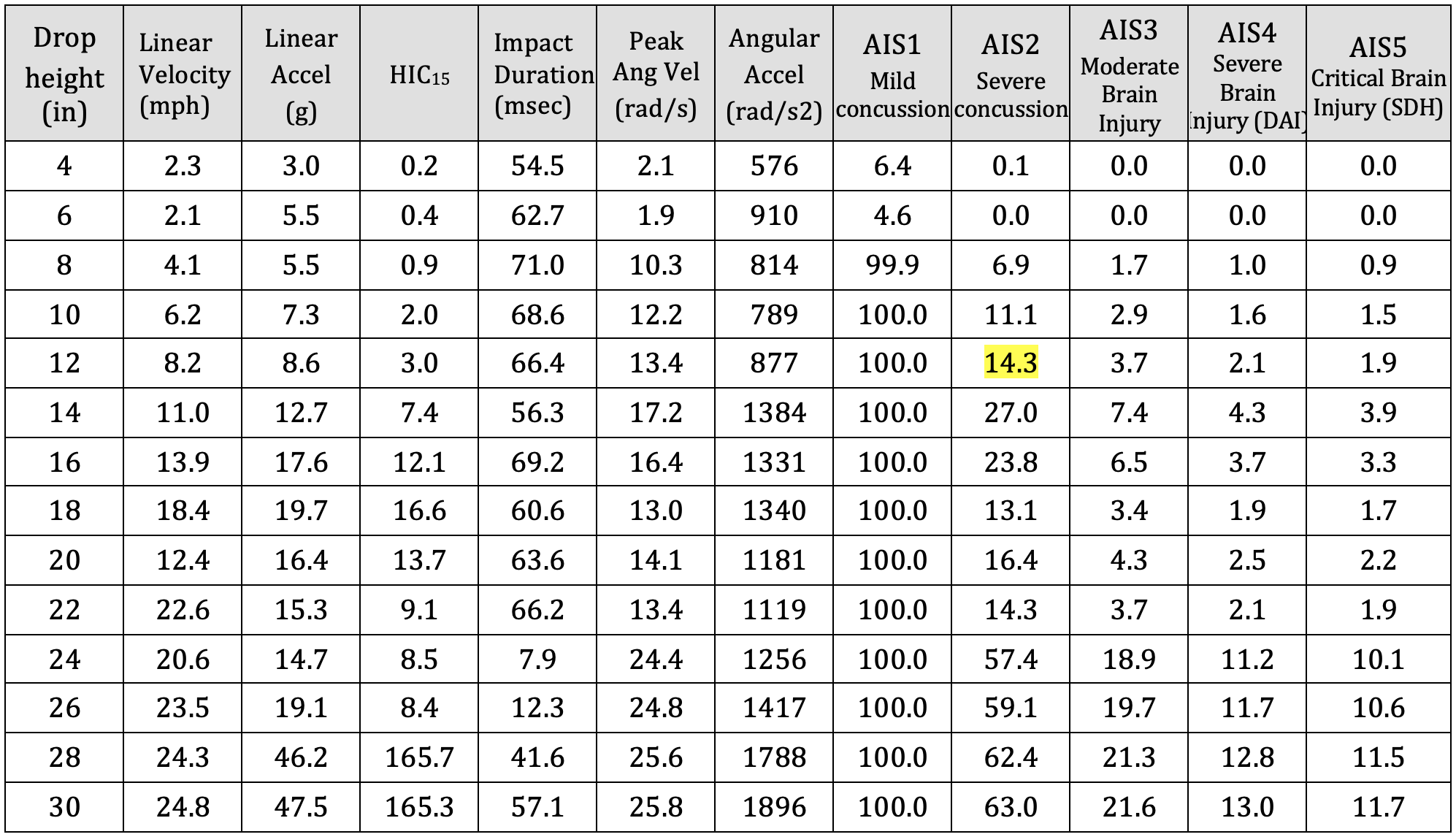
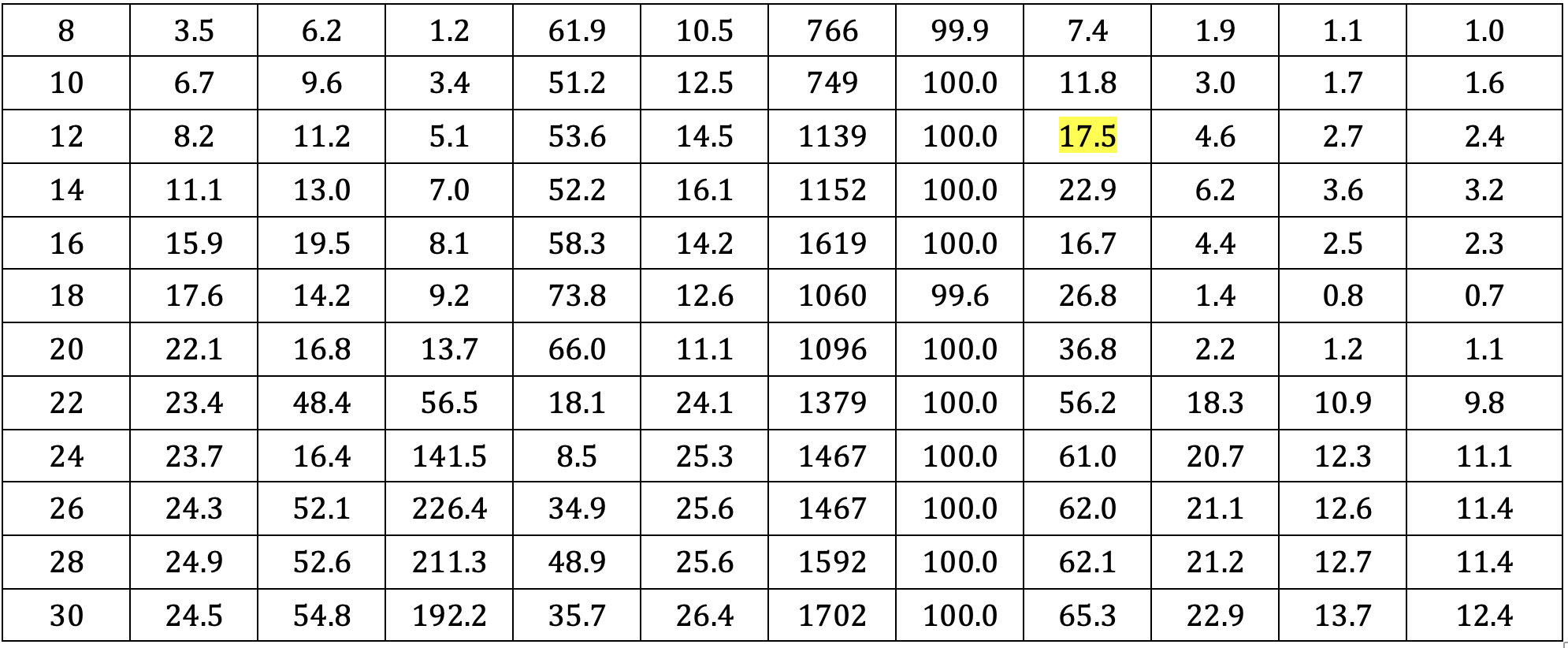
A summary of key results is presented in Table a-d, below. The driver was aware of the pending impact, as he depressed the accelerator in an attempt to avoid the collision in the moments prior to the crash. In rear end collision tests involving human subjects, volunteers instinctively tensed their neck muscles as a protective response. Given that the driver anticipated the crash his neck muscles were likewise expectedly tense as an instinctive protective response. Therefore, the results most consistent with the subject case are presented in Tables a and b. Rows highlighted in green are consistent with change in velocity experienced by the driver during the subject crash.
Table a: Summary of test results – Neck – Stiff; Headrest – lower position
Table b: Summary of test results – Neck – Stiff; Headrest – upper positio
Table c: Summary of test results – Neck – Loose; Headrest – lower position
Table d: Summary of test results – Neck – Loose; Headrest – upper position
Skull Fracture
With reference to Ono 8, none of the impact tests approached the occipital skull fracture threshold of 140 g for impacts lasting longer than 7 milliseconds. Therefore, vehicle headrests provide excellent protection against acute skull fractures at impact speeds below 25 mph.
Traumatic Head Injury
With reference to Figure 7 and Tables a-d, maximum recorded HIC values were consistent with a 5 percent or less risk of moderate traumatic head injury. Whereas, the HIC value computed at impact speeds similar to the crash was only 3.4, at which the risk of minor or moderate traumatic head injury is negligible.
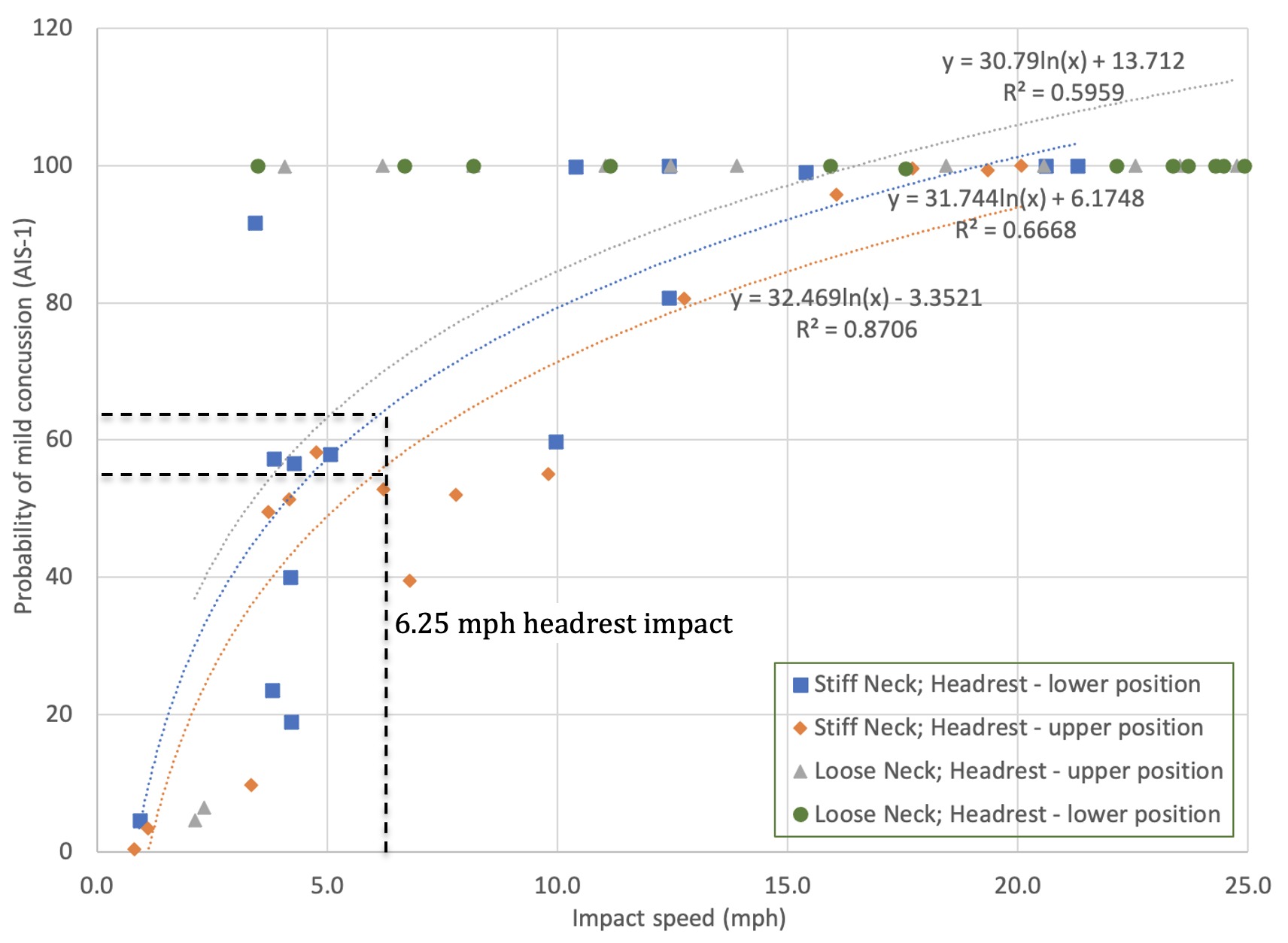
Mild Concussion
With reference to Figure 8 below, the risk of an occupant sustaining a mild concussion in a rear-end collision producing a change in velocity of 6.25 mph (range 5.4 to 7.2 mph) can be determined based on the following calculation: Risk AIS-1 = 31.744*ln(x) + 6.1748 (R2=0.67). The risk of and AIS-1 mild concussion, without post-concussion syndrome, in such an impact is 64.3% (range 59.7 to 68.8%).
Figure 8: Risk of mild concussion (AIS-1) associated with headrest impact
Severe Concussion
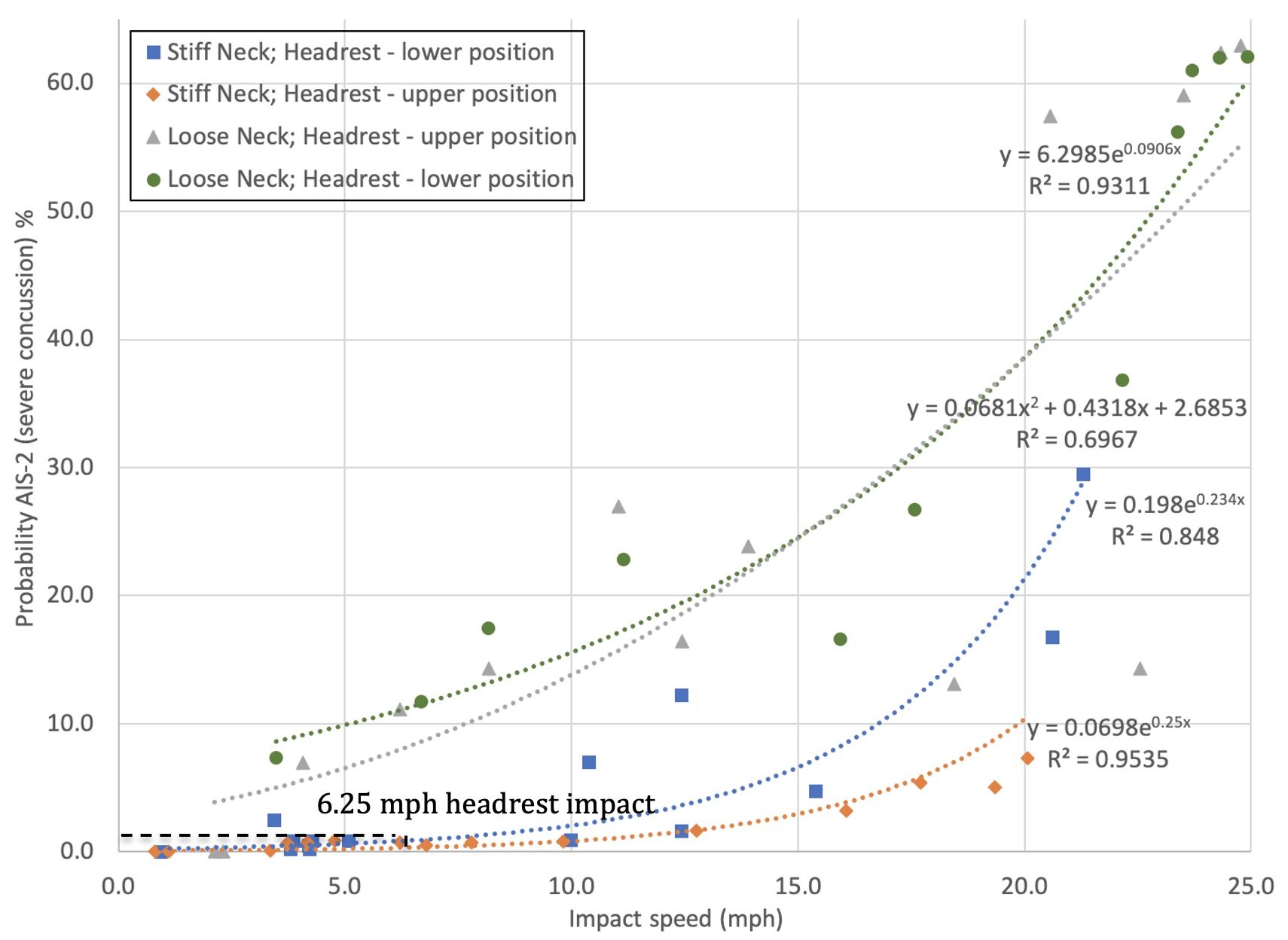
With reference to Figure 9, below, the risk of an occupant sustaining a severe concussion in a rear-end collision producing a change in velocity of 6.25 mph (range 5.4 to 7.2 mph) can be determined based on the following calculation: Risk AIS-2 = 0.198e0.234x (R2=0.85). The risk of severe concussion in such an impact is 0.85% (range 0.70 to 1.07%).
Figure 9: Risk of severe concussion (AIS-2) associated with headrest impact
Traumatic Axonal Injury:
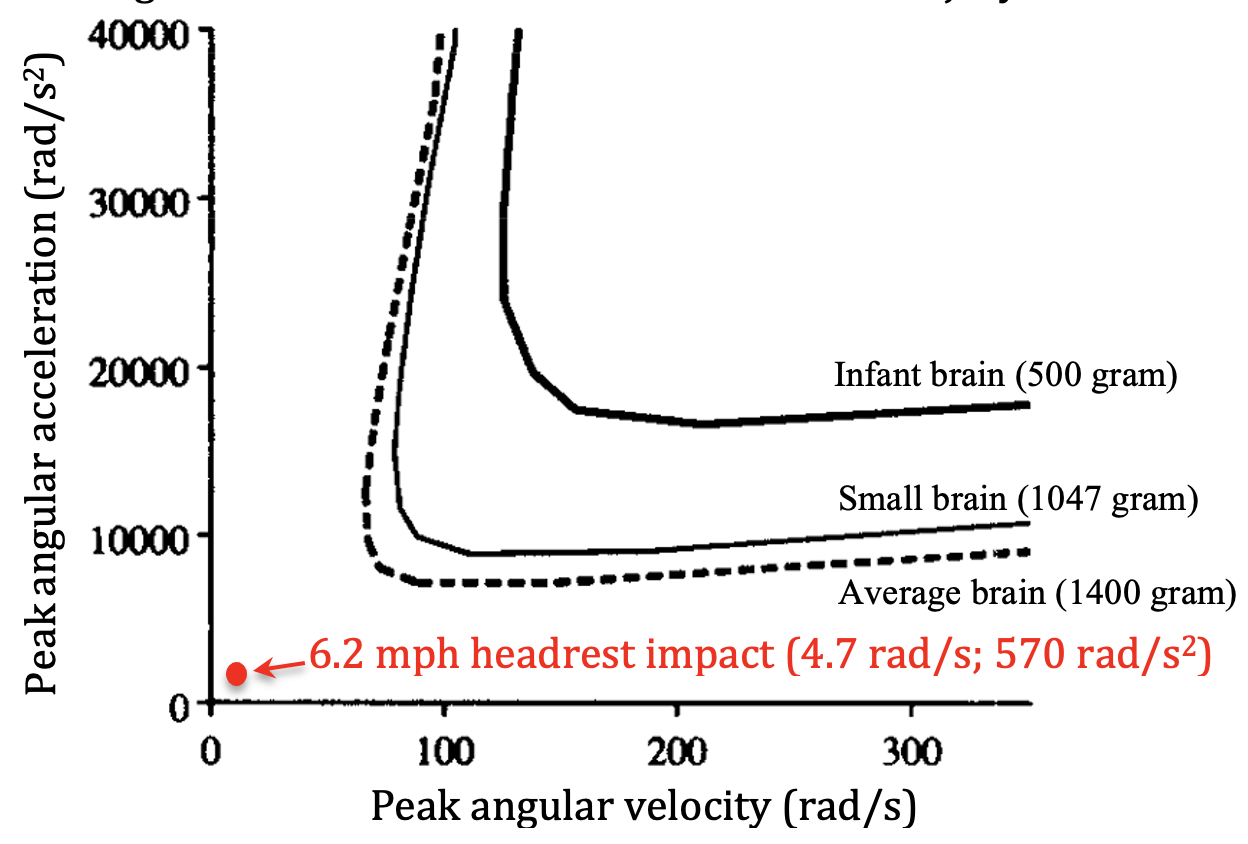
Figure 10, below, is adapted from Margulies et al. 20 in which thresholds for axonal injury were developed and published based on mathematical modeling, animal testing and physical experiments. Results from occipital head impact against an exemplar headrest at a speed of 6.2 miles per hour are represented, indicating that rotational head and brain kinematics associated with such impact are well below scientifically-accepted thresholds for traumatic axonal injury.
Figure 10: Scientific Thresholds for Axonal Injury
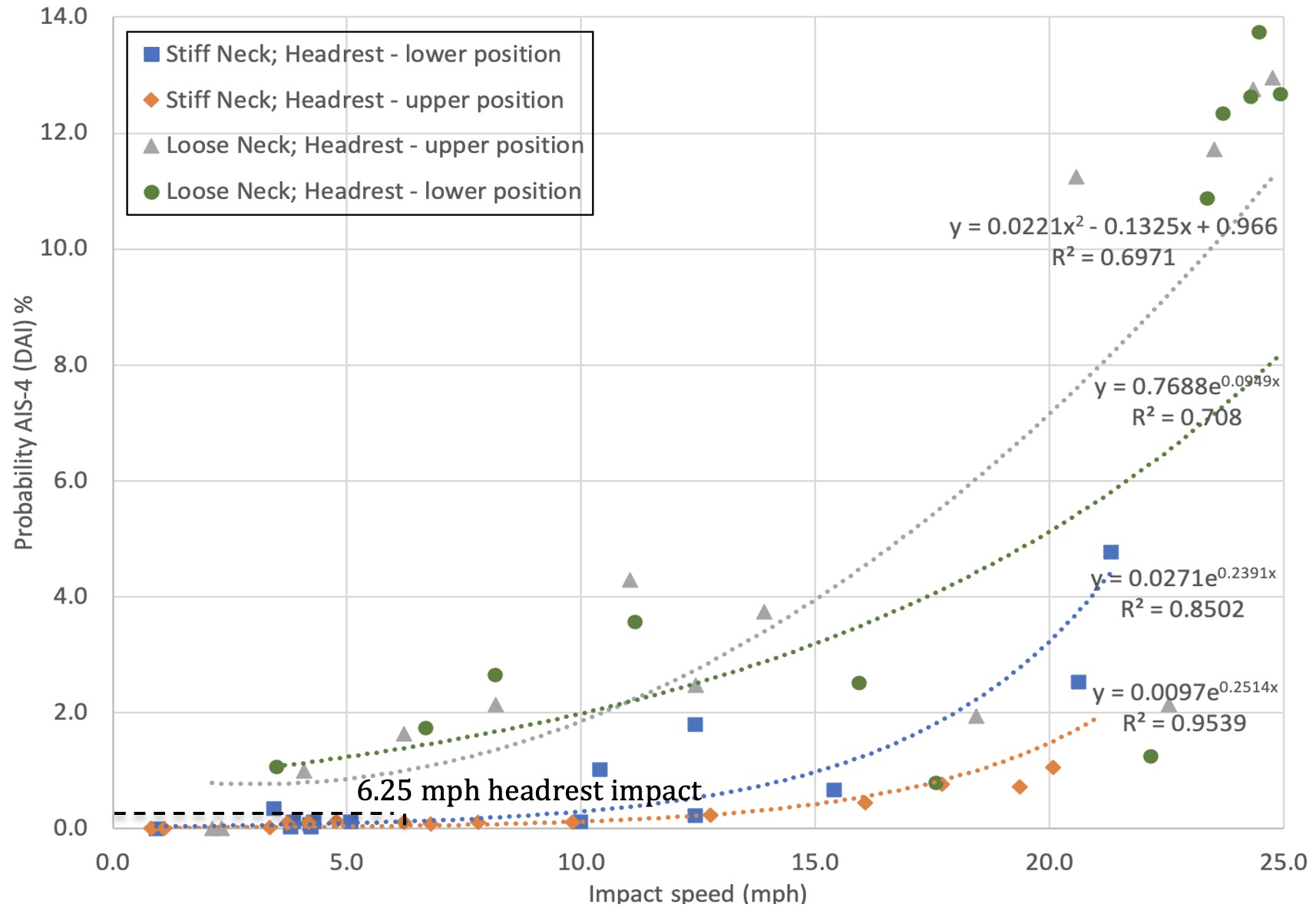
Figure 11, below was generated from data presented in Tables a through d, to present the risk of traumatic axonal injury associated with head impact against an headrest.
Figure 11: Risk of traumatic axonal injury (AIS-4) associated with headrest impact
Results show that the risk of an occupant sustaining traumatic axonal injury in a rear-end collision producing a change in velocity of 6.25 mph (range 5.4 to 7.2 mph) can be determined based on the following calculation: Risk AIS-4 = 0.0271e0.2391x (R2=0.85). The risk of traumatic axonal injury in an impact of the magnitude experienced by the driver is 0.12% (range 0.10 to 0.15%).
Conclusions
Biomechanical testing of head and brain injury risk associated with occipital head impact against a headrest, in accordance with published methods, shows a significant risk (59.7 to 68.8%) of AIS-1 mild concussion, without post-concussion syndrome, in a 6.2 mph rear-end collision. However, the risk of an AIS-2 severe concussion in such an impact decreases to 0.70 to 1.07%, and the risk of traumatic axonal injury is only 0.10 to 0.15%. Moreover, the mechanical traumatic axonal injury is not consistent with a sagittal plane impact.
References
[1] Caccese V, Lloyd J, Ferguson J (2014) An Impact Test Apparatus for Protective Head Wear Testing Using a Hybrid III Head-Neck Assembly. Experimental Techniques.
[2] Lloyd J & Conidi F. (2015). Brain Injury in Sports. Journal of Neurosurgery. October.
[3] Lloyd J. (2017). Biomechanical Evaluation of Motorcycle Helmets: Protection Against Head and Brain Injuries.Journal of Forensic Biomechanics.
[4] SAE (2014) J211/1. Instrumentation for Impact Test – Part 1 – Electronic Instrumentation. Society of Automotive Engineers International, Surface Vehicle Recommended Practice, Warrendale, PA.
[5] Padgaonkar AJ, Krieger KW and King AI. Measurement of Angular Acceleration of a Rigid Body using Linear Accelerometers. J Applied Mechanics. Sept 1975.
[6] Takhounts EG, Craig MJ, Moorhouse K, McFadden J (2013) Development of Brain Injury Criteria (BrIC). Stapp Car Crash Journal 57: 243-266.
[7] Abbreviated Injury Scale (2008) Association for the Advancement of Automotive Medicine, Des Plaines, IL.
Dr. John Lloyd recently conducted a biomechanical study to evaluate motorcycle helmets in terms of their ability to provide protection against traumatic head and brain injuries. Motorcycle helmet testing proves inadequate protection against concussion and diffuse traumatic brain injuries associated.
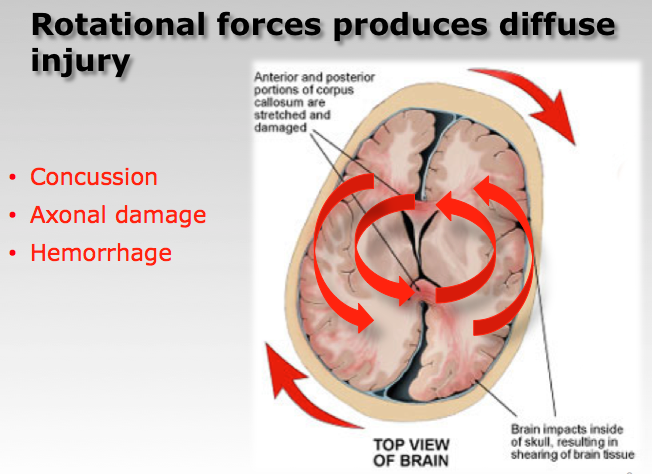
Motorcycle accident victims account for more than 340,000 fatalities annually, with the United States ranking 8th highest worldwide in the number of motorcycle accident deaths. 75% of all fatal motorcycle accidents involve brain injury, with rotational forces acting on the brain the primary cause of mortality. Current motorcycle helmets are effective at reducing head injuries associated with blunt impact. However, the mechanism of diffuse traumatic brain injury is biomechanically very different.
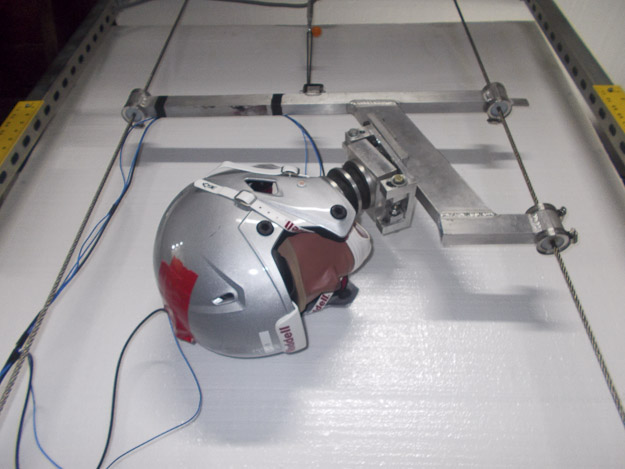
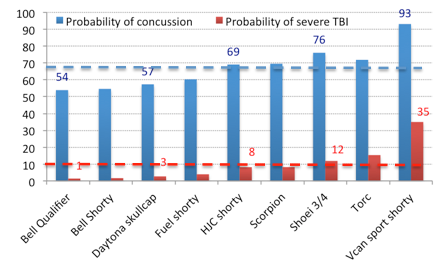
Samples of 9 motorcycle helmet models, representing full-face, three-quarter and shorty designs were evaluated. Helmets, fitted to an instrumented Hybrid III head and neck, were dropped at 13 mph in accordance with DOT motorcycle helmet testing standards.
Results show that, on average, there is a 67% risk of concussion and a 10% probability of severe or fatal brain injury associated with a relatively minor 13mph helmeted head impact.
In conclusion, motorcycle helmets provide inadequate protection against concussion and diffuse traumatic brain injuries associated with even relatively moderate impact.
To consider whether a motorcycle helmet might reduce the risk of brain trauma in a motorcycle accident it is first important to understand the two primary mechanisms associated with traumatic brain injury – impact loading and impulse loading, according to motorcycle helmet expert, Dr. John Lloyd.
Impact loading involves a direct blow transmitted primarily through the center of mass of the head, resulting in extracranial focal injuries, such as contusions, lacerations and external hematomas, as well as skull fractures. Shock waves from blunt force trauma may also cause underlying focal brain injuries, such as cerebral contusions, subarachnoid hematomas and intracerebral hemorrhages.
Whereas, impulse or inertial loading caused by sudden movement of the brain relative to the skull, produces cerebral concussion. Inertial loading at the surface of the brain can cause subdural hemorrhage due to bridging vein rupture, whereas if affecting the neural structures deeper within the brain can produce diffuse axonal injury (DAI).
Epidemiology Studies
Two major epidemiologic studies into the causation of motorcycle accidents have been conducted in North America and Europe: the Hurt Report and the MAIDS report. The Hurt Report showed that failure of motorists to detect and recognize motorcycles in traffic is the predominating cause of motorcycle accidents. Seventy-five percent of accidents were found to involve a motorcycle and a passenger vehicle, while the remaining 25% of accidents were single motorcycle accidents. Two-thirds of motorcycle-car crashes occurred when the car driver failed to see the approaching motorcycle and violated the rider’s right-of-way. Findings indicate that severity of injury increases with speed, alcohol motorcycle size and speed.
The MAIDS study (Motorcycle Accidents In Depth Study) is the most recent epidemiologic study of accidents involving motorcycles, scooters and mopeds, which was conducted in 1999 to investigate motorcycle accident exposure data across five European countries. Key findings show that passenger cars were the most frequent collision partner (60%), where 69% of the drivers report that they did not see the motorcycle and the predominance of motorcycle accidents (54.3%) occurred at an intersection.
In 1995, the European Commission Directorate General for Energy and Transport initiated a Cooperative Scientific and Technical Research (COST) program to investigate Motorcycle Safety Helmets. Several agencies from Finland, the United Kingdom, France and Germany participated in this study, which compiled and analyzed data from 4,700 motorcycle fatalities in Europe, each year. The COST report documents that 75% of all fatal motorcycle accidents involve head injury. Linear forces were present in only 31% of fatal head injuries, while rotational forces were found to be the primary cause in over 60% of cases. Within the scope of this study experiments were performed using drop tests with accelerometers to measure linear and rotational accelerations of the brain and skull mass associated with different types of impacts. These tests confirmed rotational acceleration to be a primary cause of brain injury in helmeted motorcycle accidents.
While the motorcycle helmet is currently the most effective means of protection for riders, data suggests that motorcycle helmets are only 37-42% effective in preventing fatal injury. By reducing the effects of blunt trauma to the head it is generally believed that risk of brain injury, including concussion, axonal injury and hematoma would also be reduced. However, the mechanisms of head and brain injury are very different. New research shows that these mechanisms are poorly coupled, contrary to previous beliefs.
Summary
Motorcycle helmet expert report that rotational forces acting on the brain are the underlying cause of traumatic brain injuries.
Motorcycle helmets, including those certified under DOT and SNELL standards are designed to mitigate forces associated with linear acceleration.
According to motorcycle helmet expert, helmets are not currently certified under either DOT or SNELL standard against their ability to protect against the angular / rotational forces.
Epidemiologic evidence from the COST-327 report indicates that motorcycle helmets do not provide adequate protection against closed head and brain injuries
New Research
Motorcycle helmet expert Dr. John Lloyd recently published a new study: Biomechanics of Motorcycle Helmets: Protection Against Head and Brain Injury. Testing proves that motorcycle helmets provide inadequate protection against concussion and severe traumatic brain injury associated with even relatively minor head impact
Helmets are intended to minimize blunt force trauma to the head, such as skull fracture, lacerations and contusions. Whereas risk of diffuse brain injuries, such as concussion, brain bleeding and axonal injuries are caused when brain tissue, nerves and blood vessels stretch and tear as the head moves suddenly but the brain lags behind. The type of brain injury is dependent on the magnitude of this strain and the time duration over which it acts on the brain.
Risk of focal head and brain injury is measured in terms of peak linear acceleration associated with impact, while risk of diffuse brain injury is measurable in terms of peak angular acceleration.
While helmets can prevent fatalities associated with penetrating head trauma, it may be argued that protection against diffuse brain injury is of paramount importance. After all, cuts, bruises and even bone fractures will heal, but brain injuries often have life long neurologically devastating effects.
Unfortunately, helmet testing standards addresses only the risk of blunt force trauma, not risk of brain injury.
Helmets may reduce the rotational forces acting on the brain. But since helmets are not currently certified according to their ability to protect against brain injury the level of protection is not standardized. Hence, it is possible to sustain catastrophic diffuse brain injuries, even while wearing a helmet.
As a biomechanics researcher, Dr. John Lloyd has dedicated his career to understanding the biomechanics of brain injuries. One objective of which is to develop a new generation of helmets for sports and motorcycling using “intelligent” materials that hold great promise for reducing the risk of traumatic brain injuries.
Dr. Lloyd’s biomechanics laboratory employs a specialized helmet testing apparatus for evaluating the risk of both head and brain injuries. This apparatus has been published in a peer-reviewer journal.
Using this apparatus, Dr. Lloyd, evaluates the linear and rotational forces associated with specific impact events, such as a motorcycle crash or sports injury, to determine whether an unhelmeted condition, or the type of helmet might have prevented the injury sustained. This apparatus has also been used to investigate whether a particular helmet failed to perform or did not meet scientifically-acceptable levels of protection.
Traditional testing of motorcycle helmets focuses on reducing the effect of linear impact forces by dropping them from a given height onto an anvil and measuring the resultant peak linear acceleration. According to the Federal Motor Vehicle Safety Standard (FMVSS) 218, commonly known as the DOT helmet standard, the test involves dropping a motorcycle helmet onto a flat steel and hemispherical anvil at an impact velocity of 6.0 m/s (13.4 mph). In general, if the resultant peak linear acceleration is less than 400G, the helmet is considered acceptable. Current motorcycle helmet testing standards do not incorporate measures of angular acceleration and therefore do not address whether any motorcycle helmet can provide protection against diffuse brain injuries, including concussion.
In 1995, the European Commission Directorate General for Energy and Transport initiated a Cooperative Scientific and Technical Research (COST) program to investigate Motorcycle Safety Helmets. Several agencies from Finland, the United Kingdom, France and Germany participated in this study, which compiled and analyzed data from 4,700 motorcycle fatalities in Europe, each year. The COST report [i] documents that 75% of all fatal motorcycle accidents involve head injury. Linear forces were present in only 31% of fatal head injuries, while rotational forces were found to be the primary cause in over 60% of cases.
Dr. Lloyd recently conducted independent testing of various motorcycle helmets utilizing a methodology that has been peer-reviewed [i] and has survived a Daubert motion for exclusion [ii]. The following figure presents peak angular acceleration results of repeated testing of various motorcycle helmets, including: (i) Voss novelty helmet, (ii) Bell shorty helmet, (iii) Daytona shorty helmet, and (iv) Bell full-face helmet, compared with an unhelmeted condition for impacts onto concrete at approximately 20mph. The red horizontal line on the figure indicates the 50% threshold for concussive trauma, as defined by Pellman et al [iii].
Results show that while a novelty or DOT approved motorcycle helmet will reduce the peak angular acceleration associated with a head impact relative to an unhelmeted condition, the level of protection is not sufficient to prevent diffuse brain injury in a typical motorcycle accident.
[i] Caccese V, Ferguson J, Lloyd J, Edgecomb M, Seidi M and Hajiaghamemar M: Response of an Impact Test Apparatus for Fall Protective Headgear Testing Using a Hybrid-III Head/Neck Assembly. Experimental Techniques, 2014.
[ii] Superior Court, Judicial District of Hartford, CT. Docket Number: HHD-CV-13-6043998-S. Case Caption: SHUMBO, JAKE Et Al v. K2 SPORTS USA Et Al. Order #227.86 regarding: 03/02/2015 Motion to Exclude Expert Testimony. Notice Issued: 07/09/2015
[iii] Pellman EJ, Viano DC, Tucker AM, Casson IR, Waeckerle JF: Concussion in professional football: reconstruction of game impacts and injuries. Neurosurgery 53(4): 799-812, 2003
[iv] COST-327 report of the European Commission Directorate General for Energy and Transport on Motorcycle Safety Helmets. (1999).
The common belief among riders is that a motorcycle helmet protects the whole head, including the brain. However testing standards in Europe (ECE 22.05) and the US (DOT & Snell), which involve dropping helmeted headforms from heights of 2-3 meters onto a steel plate, only evaluate a motorcycle helmet in terms of its ability to protect against blunt force trauma, such as skull fractures and penetrating head injuries. The mechanism underlying diffuse brain injuries, such as concussions and brain hemorrhages is distinctly different, but is not assessed by current motorcycle helmet testing standards.
Imagine a bowl of jelly, where the bowl represents the skull and the jelly represents the brain. The bowl (skull) serves to protect the jelly (brain) from impact by dispersing forces over a larger surface area. If the bowl were impacted such that the force passes through the center of the jelly, the jelly moves very little. This is called linear force. Whereas, if you rotate the bowl of jelly between your hands you will see that the jelly moves quite a lot, especially towards its center. This is called a rotational force.
In reality, most motorcycle helmet impacts will produce both linear and rotational forces. In the case of head and brain injury, linear forces are responsible for injuries such as bruises and fractures. Whereas rotational forces cause the nerves and blood vessels in the brain to stretch and tear, leading to concussions, injury to the nerve fibers (axonal trauma) and brain bleeding (hematomas).
The human head is designed to protect the brain against typical impacts associated with daily living, such as normal bumps and falls. The skull can be thought of as a helmet to the brain by resisting penetrating injury to the brain. While the scalp glides over the skull to decrease rotational forces, thereby reducing the risk and severity of diffuse brain injuries. However, the forces associated with motorcycle collisions far exceed that which the human skull and scalp was intended to protect. Hence in motorcycling the use of a helmet to reduce the risk of such injuries is typically mandated.
Helmets are designed with 3 principal components – the outer shell, the inner liner and a comfort layer. The shell is typically made of polycarbonate plastics or fiberglass and serves two purposes; to minimize the likelihood that a sharp object might penetrate the head, and to dissipate the impact over a larger surface area. The inner liner is made from EPS foam (polystyrene) and serves to absorb the impact forces. The comfort layer does nothing more than provide comfort between the head and the polystyrene liner. Unfortunately, the polystyrene liner has limited effectiveness at reducing the rotational forces – those responsible for diffuse brain injuries – below safe levels.
A cooperative study was undertaken in Europe in the late 1990s to examine motorcycle accidents and their causes. Based on data from 4,700 helmeted motorcyclist deaths, the study found head injuries accounted for three-quarters of all fatalities. More than 60 percent of which were brain injuries caused by rotational forces, while only 30 percent of fatal head injuries were due to linear forces. This extensive study proves that motorcycle helmets are inadequate in providing necessary protection against diffuse brain injuries.
One might propose that protection against diffuse brain injury ought to deserve a higher priority. After all, the skull will likely heal from trauma, but the brain may not.
The challenge with protective headgear, including motorcycle, military and sports helmets is that, due to the characteristics of the liner materials, the head is directly coupled to the helmet. That is, the head and helmet are effectively joined and move as one. Therefore upon impact, any rotational forces generated on the helmet are transmitted directly to the brain. In fact, due to the size of helmets rotational forces can actually be amplified. The solution lies in de-coupling the head from the helmet, much the way that the scalp is de-coupled from the skull, so that the helmet can have some degree of rotation independent of the head. In this way, the rotational forces are dampened before they are transmitted to the brain, thereby lessening the risk and severity of brain injury.
BRAINS, Inc., of which Dr. Lloyd is the Research Director, is developing a new generation of motorcycle helmets, utilizing a patented composite of shear-thickening non-Newtonian materials. Due to their nature, these advanced materials respond differently to linear and rotational forces, thereby allowing the helmet some independent rotational motion, effectively de-coupling the helmet from the head. This technology was demonstrated at NI Week (http://youtu.be/T591x950oRI) and shows great promise for protection against both blunt force trauma and traumatic brain injuries.
Given the choice of a helmet that protected against skull fracture and one which also provides protection against brain injury, which would you choose?
Dr. John Lloyd holds a PhD in Ergonomics from Loughborough University and is a Brain Injury Specialist. He is an expert in the field of brain injury biomechanics.
As a motorcycle enthusiast, John has clocked more than 250,000 miles and completed numerous training programs. Dr. Lloyd has served as a biomechanics expert on a variety of motorcycle accident cases.
In December a movie titled “Concussion”, staring Will Smith will be released in theaters, chronicling the work and bravery of Dr. Bennett Omalu, who first discovered Chronic Traumatic Encephalopathy (CTE) as the consequence of repeated blows to the brain in football and attempts by the National Football League (NFL) to deny any causal link.


 Analysis of one player’s self-reported concussive impact clearly shows decreased Gamma band activity and increased Theta band activity in the frontal cortex of the brain immediately following significant head impact. This suggests that the player had reduced cognitive performance and was perhaps in a ‘drowsy’ state for about 10 minutes following impact. During this time, the player may have been dazed and confused and certainly less effective on the field. But more importantly, his ability to protect himself from a second, potentially harmful impact was greatly compromised.
Analysis of one player’s self-reported concussive impact clearly shows decreased Gamma band activity and increased Theta band activity in the frontal cortex of the brain immediately following significant head impact. This suggests that the player had reduced cognitive performance and was perhaps in a ‘drowsy’ state for about 10 minutes following impact. During this time, the player may have been dazed and confused and certainly less effective on the field. But more importantly, his ability to protect himself from a second, potentially harmful impact was greatly compromised.






 Impact loading involves a direct blow transmitted primarily through the center of mass of the head, resulting in extracranial focal injuries, such as contusions, lacerations and external hematomas, as well as skull fractures. Shock waves from blunt force trauma may also cause underlying focal brain injuries, such as cerebral contusions, subarachnoid hematomas and intracerebral hemorrhages.
Impact loading involves a direct blow transmitted primarily through the center of mass of the head, resulting in extracranial focal injuries, such as contusions, lacerations and external hematomas, as well as skull fractures. Shock waves from blunt force trauma may also cause underlying focal brain injuries, such as cerebral contusions, subarachnoid hematomas and intracerebral hemorrhages.