The following is a peer-reviewed article on Motorcycle Accident Reconstruction, which was originally published in the Journal of Forensic Biomechanics in January 2016.
Corresponding author: John D Lloyd, Research Director, BRAINS, Inc., 32824 Michigan Avenue San Antonio, Florida, 33576, USA, Tel: 813-624-8986; Fax: 352-588-0688; E-mail: drjohnlloyd@tampabay.rr.com
-
Abstract
In a motorcycle accident, the motorcycle and rider typically become independent, each following their own path to final rest. Consequently, the biomechanical analysis of a motorcycle accident reconstruction is complex. A biomechanical model to assess rider kinematics associated with motorcycle accidents is presented, which may be important to forensic scientists involved in the analysis of such events. This model can also be applied to other activities, including cycling, equestrian sports, skiing, skating, running, etc.
In a motorcycle accident reconstruction, it is first important to understand the mechanisms by which a rider may be ejected from their motorcycle and how drag factors affect the motorcycle and rider independently. Next we determine rider trajectory, taking into consideration rider anthropometry and posture, results from which are used to derive impact velocity as a function of linear and angular components. A case study is presented, demonstrating how the presented model can be applied to a collision involving a single motorcycle.
-
Keywords:
Forensic science; Biomechanics; Kinematics; Anthropometry; Motorcycle accident reconstruction
-
Introduction to Motorcycle Accident Reconstruction
Motorcycles are a luxury in the developed world, where they are used mostly for recreation. Whereas in developing countries, motorcycles are required for utilitarian purposes due to lower prices and greater fuel economy. It is estimated that in 2016 there will be more than 134 million motorcycles worldwide [1], 60-80% of which are in the Asia Pacific and Southern and Eastern Asia regions. In 2011 there were more than 8.2 million registered motorcycles in the United States [2], representing 3% of all US registered vehicles, with California, Florida and Texas leading the number of motorcycles per state [3].
3.1. Epidemiology of motorcycle accidents
In the United States motorcyclists travelled 18.5 billion miles in 2011, which represents only 0.6% of total vehicle miles travelled, yet motorcyclists accounted for 14% (4,612) of traffic fatalities and 4% (81,000) of all occupant injuries [2]. According to the U.S. National Highway Traffic Safety Administration (NHTSA), when compared with automobiles, per vehicle mile traveled, motorcyclists’ risk of a fatal crash is 35 times greater than that of a car occupant [4].
Two major epidemiologic studies into the causation of motorcycle accidents have been conducted in North America and Europe: the Hurt Report and the MAIDS report. The Hurt Report [5] showed that failure of motorists to detect and recognize motorcycles in traffic is the prevailing cause of motorcycle accidents. Seventy-five percent of accidents were found to involve a motorcycle and a passenger vehicle, while the remaining 25% of accidents were single motorcycle accidents. Two-thirds of motorcycle-car crashes occurred when the car driver failed to see the approaching motorcycle and violated the rider’s right-of-way. Findings of the Hurt study indicate that severity of motorcyclist injury increase with speed, alcohol consumption, motorcycle size and speed.
The MAIDS study (Motorcycle Accidents In Depth Study) [6] is the most recent epidemiologic study of accidents involving motorcycles, scooters and mopeds, which was conducted in 1999 across five European countries to investigate motorcycle accident exposure data. Key findings show that passenger cars were the most frequent collision partner (60%), where 69% of the drivers report that they did not see the motorcycle and the predominance of motorcycle accidents (54.3%) occurred at an intersection.
In the United States alone, it is estimated that the total direct costs associated with motorcycle crashes in 2010 was approximately $16 billion. However, the US Government Accountability Office (GAO) predicts that full costs of motorcycle crashes are likely considerably higher because some difficult-to-measure costs, such as longer-term medical costs, are not included [7].
-
Biomechanical Model
A new model is presented for the purpose of investigating motorcycle accident reconstruction biomechanics involving a lone motorcycle, which accounts for 25% of all motorcycle-related accidents according to the Hurt report [5]. This model is unique in that it incorporates measures of rider anthropometry (body measurements) and riding posture, which have a direct effect on trajectory and overall height of the vertical component of the impact.
The model presented herein may be applied not only to motorcycle accidents, but also to a wide range of activities, including cycling, equestrian sports, skiing, skating, running, etc.
-
Methods
It is first important to understand the mechanisms by which a rider may be ejected from their motorcycle and how drag factors affect the motorcycle and rider independently. Next we determine rider trajectory, results from which are used to derive impact velocity as a function of linear and angular components. Finally, characteristics of the impact surface are considered with respect to impact accelerations.
5.1. Rider ejection
There are a number of ways that a rider can be ejected from the bike in a lone motorcycle accident. Two common ways of ejection are the lowside (Figure 1A) and highside (Figure 1B) crash. A rider may also be ejected over the handlebars (Figure 1C).
Figure 1 – Rider Ejected from Motorcycle
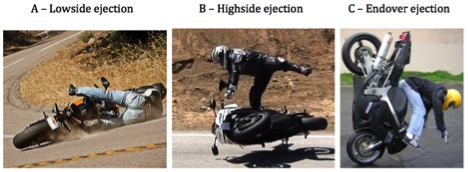
The lowsider or lowside is a type of motorcycle crash usually occurring in a turn (Figure 1A). A lowside crash is caused when either the front or rear wheel slides out as a result of either too much braking in a corner, too much acceleration through or out of a corner, or too much speed carried into or through a corner for the available traction. A lowside crash may also be caused by unexpected slippery or loose material (such as oil, water, dirt or gravel) on the road surface.
A highsider or highside is a type of motorcycle accident characterized by sudden and violent rotation of the motorcycle about its longitudinal axis. This generally happens when the rear wheel loses traction, skids, and then suddenly regains traction, creating a large torque, ejecting the rider off the side of the motorcycle, oftentimes head-first (Figure 1B).
Highside and lowside accidents differ as follows: during a lowside the rear wheel slips laterally and continuously until the motorcycle falls onto the side facing the inside of the corner.Whereas during a highside crash the rear wheel slips laterally before suddenly regaining traction and flipping the motorcycle toward the outside of the corner (the higher side of the motorcycle). Highsides happen quickly and are very violent consequently injuries tend to be more severe in a high side crash, compared to a lowside crash.
Endo, short for “end over end,” occurs when the front end of a motorcycle stays fixed while the rear rotates up into the air, causing a rider to fly over the handlebars (Figure 1C).
5.2. Drag factors
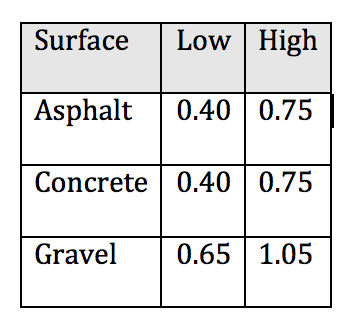
Drag factors for motorcycles have been established based on motorcycle accident reconstruction and typically range from 0.2-1.0 [8], where 0.25 represents a motorcycle with a fairing [9], such as a sport motorcycle. Sport and sport touring motorcycles will likely slide further than a cruiser-style motorcycle, which have more external components that resist sliding, for which a drag factor of 0.5 is commonly adopted Table 1, below, presents drag factors for street motorcycles sliding on typical road surfaces [10-13].
Table 1: Drag Factors for Sliding Motorcycles
Drag factors for the rider are typically higher than those for motorcycles sliding on a dry asphalt or concrete roadway. An extensive series of motorcycle accident reconstruction tests were carried out by the West Midlands Police in the United Kingdom in which they calculated the drag factor value of a crash-test dummy sliding across an airfield surface. The resulting coefficient was found to vary between 0.57 and 0.85 for normal clothing [14].With similar drag factors for dry and wet roadway conditions [15]. For the purpose of accident reconstruction, a drag factor of 0.7 for a clothed individual sliding on a roadway is generally accepted.
Evidence from final rest positions of the motorcycle and rider can be used to establish whether the rider was involved in a lowside or highside motorcycle ejection. In a lowside crash the motorcycle will tend to slide further than the rider. Whereas in a highside crash, the rider is ejected from the motorcycle, traveling additional distance over ground in a similar direction to the motorcycle, prior to making contact with the ground and initiating the slide. Hence, in a highside crash, the final rest position of the rider may be beyond the final rest position of the motorcycle. Furthermore, in higher-energy ejection crashes the rider is more likely to both slide and tumble, resulting in a longer travel distance from location of ejection from the motorcycle, as well as additional injuries as evidenced by fractures, lacerations and contusions to various regions of the body.
5.3. Rider anthropometry
Anthropometry is the study of human body measurements. Rider anthropometry will directly affect fall height, since head center of mass (HCOM) and overall center of mass (RCOM) varies between individuals.
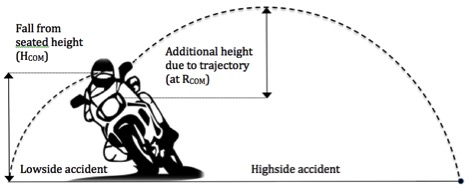
In a lowside crash, seated height of the center of mass (HCOM) of the rider’s head approximates vertical fall height. Whereas in a highside crash vertical fall height is a function of seated head CoM height (HCOM), plus additional height gained based on trajectory of the rider calculated with reference to overall center of mass of the rider (RCOM) (Figure 2).
Figure 2 – Fall Height Associated with Low side and High side Accidents
5.4. Rider center of mass
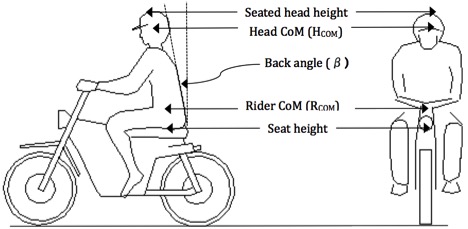
Rider center of mass height (RCOM) is located anatomically with respect to the second sacral vertebra (S2), which can be visually estimated as approximate in height to the omphalion (navel), and is measured vertically with respect to the road surface. The preferred method for determining RCOM is to measure seated height of the rider on the subject motorcycle (Figure 3). If the rider is not available due to injury or fatality, then an exemplar same-gender person of similar height and weight may be used. If the subject motorcycle is not available due to extent of damage, then an exemplar motorcycle should be obtained. With the motorcycle supported perpendicular to the road by an assistant (not on side stand or center stand), and rider’s hands on the handlebar grips and feet on the foot pegs, measure the vertical height from the ground to the motorcycle seat at the location of the ischial tuberosities (base of the pelvic bones at the seat surface). An anthropometer and spirit level should ideally be used for accuracy and measurements recorded in millimeters to maximize precision.
Figure 3 – Rider anthropometry
As an alternative method, rider seated height can be calculated by sourcing motorcycle seat height, from manufacturer specifications, from which a correction factor for suspension compression under mass of the rider is subtracted. Suspension compression, also known as sag, will vary by motorcycle type and mass of the rider. A general rule of thumb is that the front sag should be about 30-35% of travel, while the rear should be at about 25%, which equates to 30-40 mm at the front and 25-35 mm at the rear for most bikes [16]. Therefore, a reasonable correction factor for suspension sag is 30-35 mm.
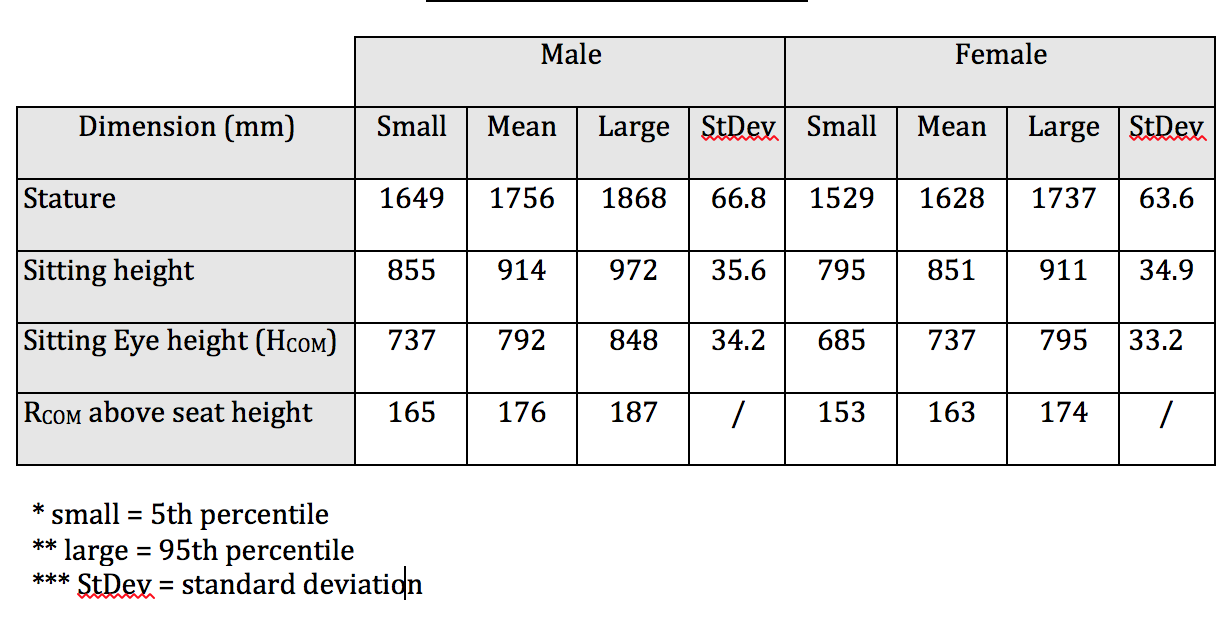
For both methods, an adjustment must be added to the compressed seat height to determine RCOM. According to Pheasant [17], seated RCOM is equal to seat height plus 10% of total stature (standing height). This factor calculation is identical for both males and females (Table 2).
Table 2: Anthropometric Data
5.5. Head center of mass
Head center of mass (HCOM) height can also be measured directly using the method described earlier, with the rider seated on the subject motorcycle in the correct riding position. An anthropometer is used to measure the vertical height from the ground. If the rider and/or subject motorcycle is unavailable, a substitute individual of similar height and weight and exemplar motorcycle may be used. The canthus (outer corner of the eye) is used as an anatomical landmark reference, equal in height to the center of mass of the head (Figure 3).
Alternatively, seated head center of mass (HCOM) can be calculated as a function of stature (standing height). Utilizing data from the 1988 Anthropometric Survey of U.S. Personnel [18], HCOM is derived by multiplying stature by 45.2%. Similar to the RCOM calculation, HCOM must be corrected for posture by multiplying HCOM by the cosine of seated back angle (β), measured with respect to the vertical axis.
5.6. Trajectory of the rider
The trajectory is the path that a rider is thrown or vaulted under the action of gravity, neglecting all other forces, such as friction from air resistance, without additional propulsion (Figure 4) and is defined by Equation 1.
Equation 1 – Trajectory of the ejected rider (y): 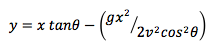
Figure 4 – Trajectory of an Ejected Rider
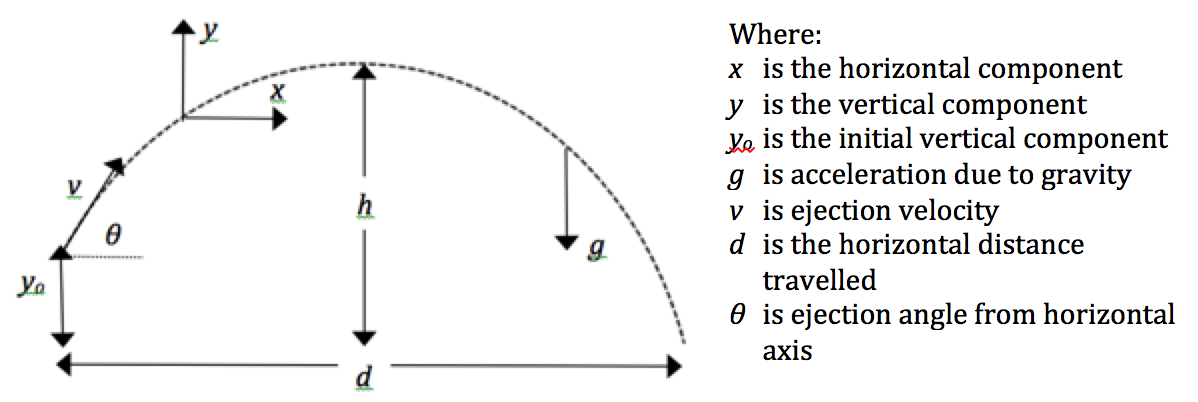
The following standard mathematical formulae are used to determine specific components of trajectory that are pertinent to the kinematic analysis of a rider ejected from a motorcycle.
5.7. Distance travelled
In a motorcycle accident reconstruction it may be possible to establish the actual distance of ejected travel of the rider, based upon location of ejection, typically between the end of any tire skid marks and start of gouge marks on the roadway, and location of bodily impact with the ground, identified by helmet paint transfer and/or identification of clothing fibers or body tissue on the roadway consistent with the rider. If the speed of the motorcycle at ejection (νejection) is also known, then the distance travelled (d) can be computed using the formula below, taking into account any correction factors for relative change in road height from location of ejection to impact.
Equation 2 – Horizontal distance traveled (d):![]()
However, the location of bodily impact is often difficult to identify, in which case reasonable assumptions may be made, including utilization of an estimated ejection angle (θ).
5.8. Maximum height
One of the most critical factors for determination of total impact velocity in a motorcycle accident reconstruction is the maximum height attained by an ejected rider, which is calculated according to
Equation 3 – Maximum height (h):![]()
5.9. Ejection angle
The ejection angle (θ) is the angle at which a rider must be launched in order to travel a certain distance, given the initial velocity. Oftentimes, based on the final rest positions of the motorcycle and rider and in consideration of appropriate drag factors, it is possible to approximate rider ejection velocity. Air resistance is considered negligible, therefore angle and velocity at ejection are considered equal to the angle and velocity at impact.
Equation 4 – Ejection angle (θ):![]()
5.10. Rider impact velocity
Total impact velocity is derived on the basis of its vertical, angular and travel velocity components.
5.11. Linear vertical impact velocity
Vertical impact velocity is computed as a function of seated head height, plus any additional height gained due to rider ejection from the motorcycle. The potential energy (P.E.) at any point will depend on the mass (m) at that point and its distance above the ground (h), multiplied by the gravitational acceleration constant (g) (Figure 5).
Figure 5 – Potential Energy of a Motorcyclist
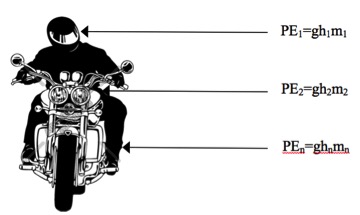
The potential energy of the entire system is the integral of the energies of each finite mass element of the motorcycle plus rider over its height: . For simplification, we assume that the mass is evenly distributed over the system. Hence, P.E=m g h.
In physics, the law of conservation of energy governs that energy can neither be created nor destroyed, Potential Energy (P.E.) at the start of a fall must be equal to the Kinetic Energy (K.E.) at the end of the fall, which is expressed as the product of one half mass (½m) and impact velocity squared (v2). Therefore P.E. = K.E. = ½ mv2, Solving for linear impact velocity gives Equation 5:
Equation 5 – Linear impact velocity:
 5.12. Angular vertical impact velocity
5.12. Angular vertical impact velocity
In real-world scenarios a falling rider will not follow a purely linear path [19], especially when coupled to a rigid body such as a motorcycle, hence angular velocity will also be generated (Figure 6).
Figure 6 – Falling Motorcyclist
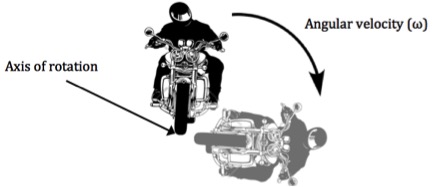
If a motorcyclist falls from a vertical to a horizontal position, we can assume that Potential Energy (P.E.) is converted to rotation: 1/2 m g h = ½ I ω2 where is the Moment of inertia, defined as the ratio of the angular momentum (L) of a system to its angular velocity (ω) around an axis: I=L/w which may also be expressed in terms of its mass (m) and its distance (r) from the pivot point as: I=mr2. Since r = h, the equation can be rewritten: mgh=1/2mh2w2. Instantaneous angular velocity at impact can be expressed in terms of linear components: ν = ω h, thus mgh=1/2mv2 which yields Equation 6:
Equation 6 – Instantaneous velocity due to angular rotation upon impact:![]()
Hence total impact velocity is the sum of its linear and angular components.
Therefore, the sum of impact velocity due to linear and angular components is greater than impact velocity due to linear components only and is expressed as:
Equation 7 – Impact velocity:
 5.13. Travel impact velocity
5.13. Travel impact velocity
As previously stated, air resistance during a short fall is considered negligible, therefore angle and velocity at ejection (α, νejection) is considered equal to the angle and velocity at impact. Velocity due to ejection can be expressed in terms of its vertical and horizontal components . Assuming that ejection angle is measured with reference to the horizontal axis, then:
Equation 8a – Vertical ejection velocity: ![]() , and Equation 8b – Horizontal ejection velocity:
, and Equation 8b – Horizontal ejection velocity:![]()
5.14. Impact velocity vector
The impact velocity vector has both vertical and horizontal components. The total vertical velocity is the sum of the linear and angular velocity components, plus the vertical components of velocity due to ejection. The total horizontal velocity will equal the horizontal component of velocity due to ejection. The magnitude of the impact velocity vector will be the square root of the sum of its vertical and horizontal components, hence:
Equation 9 – Impact velocity vector:![]()
and the effective angle of the impact velocity vector relative to the vertical axis is determined as:
Equation 10: Effective impact angle:
5.15. Impact acceleration
In a motorcycle accident reconstruction, impact acceleration is determined as a function of rate of change of impact velocity over time (t): , where the duration of the impact will be directly affected by the stopping distance of the impacted material. Roadside materials, such as grass or dirt inherently have larger stopping distances than typical roadway materials, such as asphalt or concrete. Hence, the impact accelerations experienced by a rider landing on a grassy area will be considerably less than if they impacted the roadway.
-
Motorcycle Accident Reconstruction Case Study
A cruiser motorcycle was traveling along a divided highway, approaching an intersection, when a slow-moving automobile made an abrupt unanticipated lane change immediately in front of the motorcycle. The rider applied the brakes, locking up the rear wheel, causing the motorcycle to skid. The motorcyclist swerved in an attempt to avoid contact with the automobile. The left motorcycle footplate struck the rear corner of the automobile at an impact speed of 7.2 m/s (16 mph), causing the motorcycle to rotate violently about its long axis until the tires gained traction and the rider was thrown from the motorcycle. The final resting position of the rider was 4.6 m (15 ft.) past the final resting position of the motorcycle, to which the rider slid approximately 3.7 m (12 ft.) after being vaulted approximately 6.1 m (20 ft.) from the motorcycle (Figure 7).
Figure 7 – Case study: Automobile Avoidance Collision
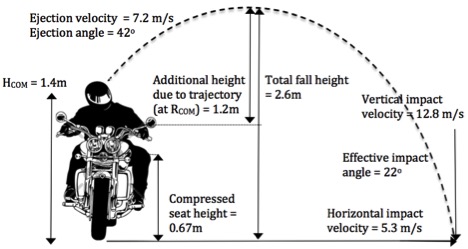
The rider center of mass was calculated based on anthropometric derivation from known standing height of 1.7 m (5’8”) and manufacturer’s seat height specification of 0.7 m (27.5”), from which a suspension compression factor of 30 mm (1.2”) was subtracted. Head center of mass was calculated to be 1.45 m (57”). Given a minimal back angle correction factor, based on rider position on a cruiser motorcycle, the corrected HCOM was 1.4 m (55”).
Based on the distance that the rider was thrown and given an ejection velocity of 16 mph an ejection angle of 42 degrees was computed in this motorcycle accident reconstruction. Hence, it was determined that the rider gained an additional height of 1.2 m (39”) due to ejection, which is added to the rider head center of mass height of 1.4 m (51”), for a total fall height of 2.6 m (8’6”). Using equation 7, an impact velocity of 8.0 m/s (18 mph) was calculated for the rotating fall. Since impact velocity and angle is assumed identical to ejected velocity and angle, travel velocity expressed in terms of its vertical and horizontal components, are 4.8 m/s (10.7 mph) and 5.3 m/s (11.9 mph), respectively. Therefore, the total impact velocity vertical and horizontal components are (8.0 + 4.8) = 12.8 m/s (28.7 mph) and 5.3 m/s (11.9 mph), respectively, with an effective impact angle of 22 degrees relative to the vertical axis.
The helmeted motorcyclist impacted an asphalt roadway, head first. Given the inherently very short stopping distance of such materials, the duration over which the impact velocity was experienced was very short, resulting in high impact accelerations, which produced life-threatening traumatic brain injuries.
The results computed by our motorcycle accident reconstruction model were validated by and corroborated based upon physical evidence from the accident scene as well as the physical evidence of the injuries sustained by the rider.
-
Conclusions
The motorcycle accident reconstruction model presented herein has been successfully applied to a typical case study involving a single motorcycle collision. Measures of rider anthropometry were incorporated into the model. In the presented motorcycle accident reconstruction case study, the rider’s stature was smaller than that of an average male and seat height was lower than most stock motorcycles. Had average male stature and average motorcycle seat height been utilized, such assumptions would have over-estimated total fall height, thereby producing a calculated vertical impact velocity greater than was actually realized. In certain circumstances, specifically where ejection angle approaches 45 degrees, a simplified model without correction for rider anthropometry and rider posture might produce results that are in disagreement with physical evidence from the accident scene. However, this improved model is not without limitations. Specifically, if a rider were leaning the motorcycle considerably at the time of loss of control, such as when cornering, the initial vertical component (yo) would be reduced. This lean angle could be estimated given the radius of the corner and if the initial speed of the motorcycle can be computed. Overall, the validation of our new motorcycle accident reconstruction model is demonstrated in its application to the motorcycle accident reconstruction case study, which is in agreement with physical evidence from the accident scene.
8. References
[1] RnR Market Research (2014) Market Research Reports Press Release: Global motorcycles market demand to rise 7.2% annually to 2016. Published July 31.
[2] National Safety Council (2013) Injury Facts – 2013 Edition. Itasca, IL..
[3] Statista – The Statistics Portal. U.S. motorcycle registrations in 2012, by state http://www.statista.com/statistics/191002/number-of-registered-motorcycles-in-the-us-by-state/ accessed 12/23/2015.
[4] NHTSA’s National Center for Statistics and Analysis (2007) Motorcycles Traffic Safety Fact Sheet (DOT-HS-810-990), 1200 New Jersey Avenue SE, Washington, DC 20590: National Highway Traffic Safety Administration.
[5] Hurt HH, Ouellet JV, Thom DR (1981) Motorcycle Accident Cause Factors and Identification of Countermeasures. Volume 1: Technical Report. University of Southern California Traffic Safety Center, Los Angeles, CA..
[6] ACEM (2000) MAIDS (Motorcycle Accidents In Depth Study): In-depth investigations of accidents involving powered two wheelers – Final Report. European Association of Motorcycle Manufacturers, Brussels..
[7] U.S. Government Accountability Office (2012) Motorcycle Safety: Increasing Federal Funding Flexibility and Identifying Research Priorities Would Help Support States’ Safety Efforts. Report number GAO-13-42.
[8] Obenski KS (1994) Motorcycle Accident Reconstruction: Understanding Motorcycles. Lawyers & Judges Publishing Co., Tucson, AZ..
[9] Medwell C, McCarthy J, Shanahan M (1997) Motorcycle Slide to Stop Tests. SAE Technical Paper 970963., SP-1237 Accident Reconstruction and Animation VII, Warrendale, PA
[10] Southwestern Association of Technical Accident Investigators (1984) Motorcycle Drag Factor Tests. Phoenix, AZ.
[11] Day TD, Smith JR (1984) Friction Factor for Motorcycles Sliding on Various Surfaces. SAE paper 840250. Society of Automotive Engineers, Warrendale, PA.
[12] Iowa State Patrol (1985) Motorcycle Test Skidding on its Side, Traffic Investigation Spring Seminar. Johnston, IA..
[13] Royal Canadian Mounted Police (1984) Motorcycle Testing. Coquitlam, BC, Canada.
[14] Hague DJ (2001) Calculation of Impact Speed from Pedestrian Slide Distance. Proceedings of The Institute of Traffic Accident Investigators International Conference
[15] Searle JA, Searle A (1983) The Trajectories of Pedestrians, Motorcycles, Motorcyclists, etc., Following a Road Accident. SAE paper 831622.. Society of Automotive Engineers, Warrendale, PA.
[16] Thede P, Parks L (2010) Race Tech’s Motorcycle Suspension Bible. Motorbooks International publisher, UK. Cd s.
[17] Pheasant, S. (1998) Bodyspace. Taylor and Francis, London.
[18] Gordon CC, Churchill T, Caluser CE, Brandtmiller CB, McConville JT et al. (1989).1988 Anthropometric Survey of US Army Personnel. US Army Technical Report TR-89/044. Natick, MA.
[19] Barnett, RL (1995) The drunk, the child and the soldier – my how they fall. Triodyne Inc. Safety Bulletin. ISSN 1081-4140. Vol 2 (2).
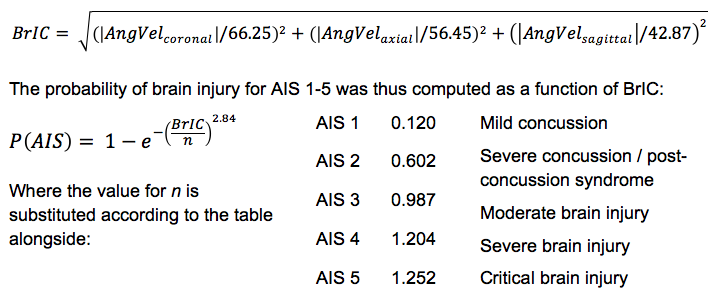
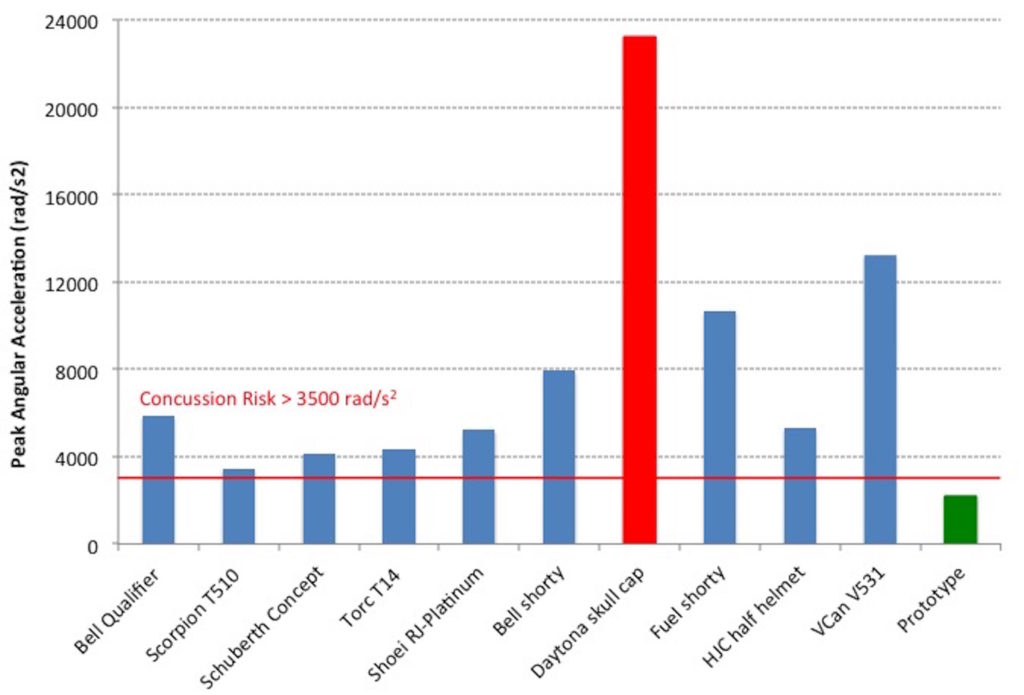
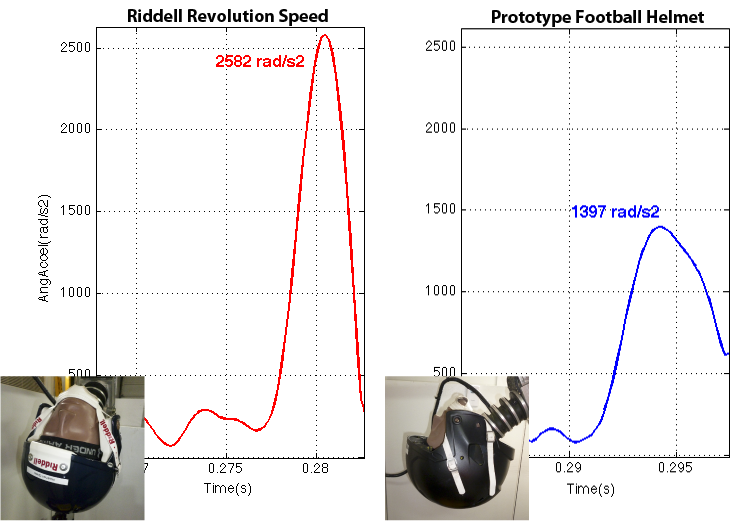
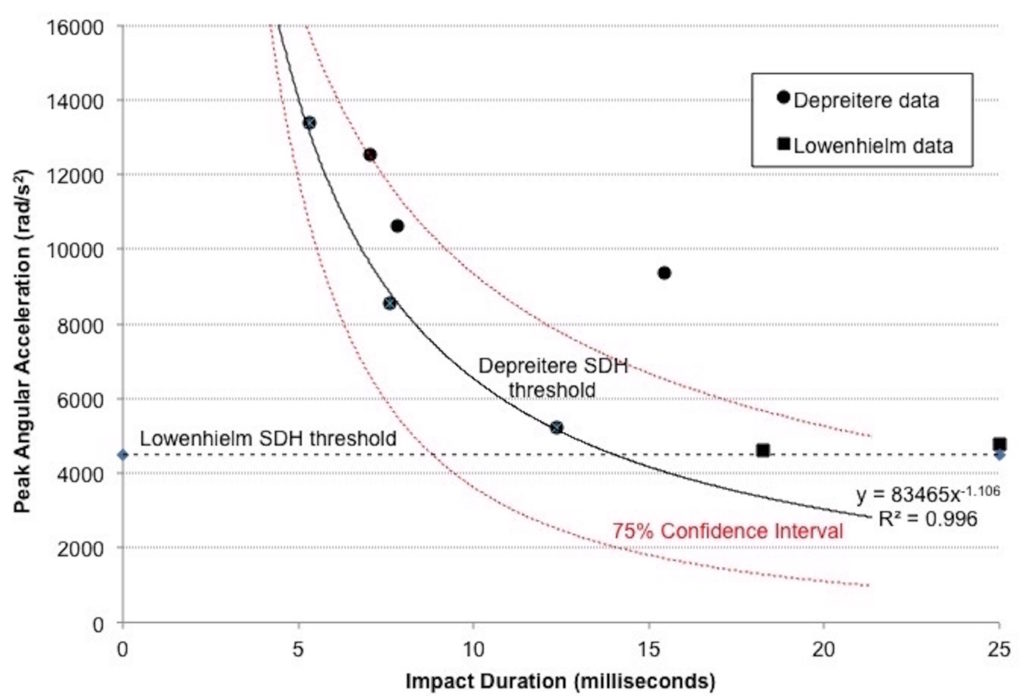 Helmets decrease peak translational force by extending the impulse duration. In the case of motorcycle helmets, typical impulse duration is approximately 12 milliseconds. With reference to Figure 1, above, this suggests that bridging vein rupture may result with peak angular accelerations in the order of 5,000 rad/s2, but may be as low as 3,000 rad/s2 after adjusting for standard error of the mean in this limited dataset.
Helmets decrease peak translational force by extending the impulse duration. In the case of motorcycle helmets, typical impulse duration is approximately 12 milliseconds. With reference to Figure 1, above, this suggests that bridging vein rupture may result with peak angular accelerations in the order of 5,000 rad/s2, but may be as low as 3,000 rad/s2 after adjusting for standard error of the mean in this limited dataset.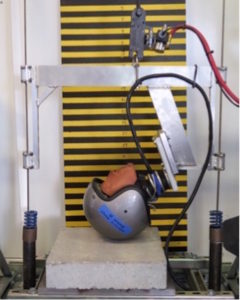

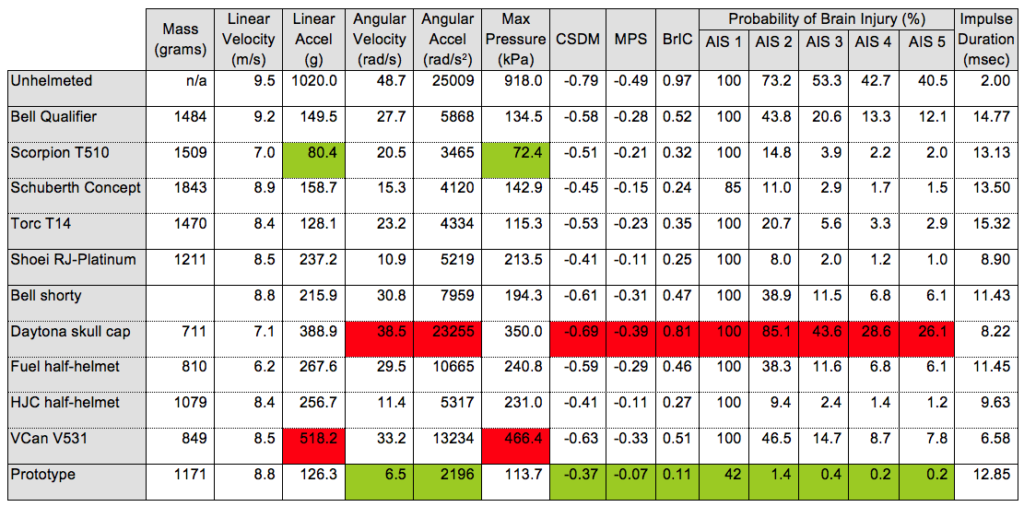
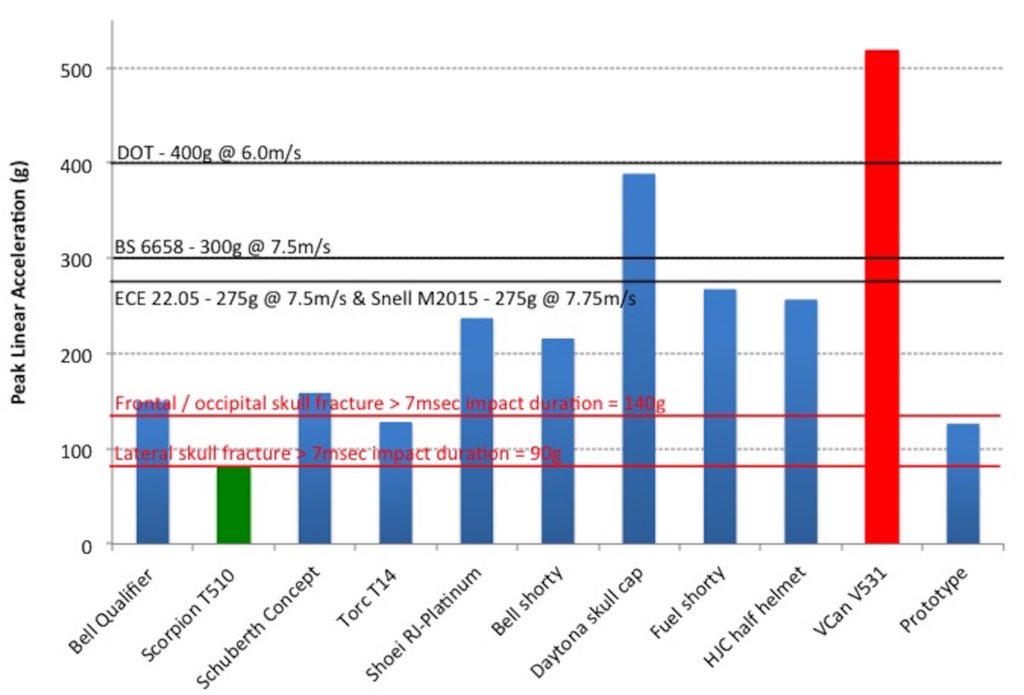
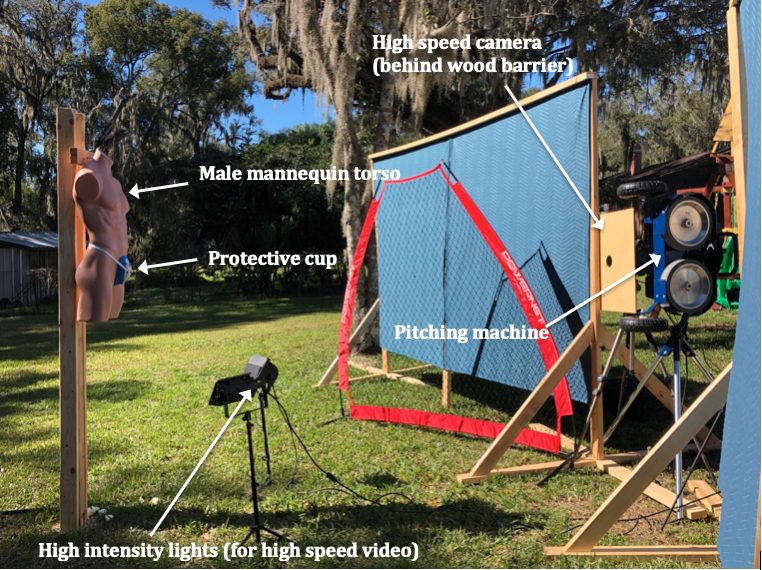
 Five samples of each motorcycle helmet model were purchased in new condition. Each helmet was impacted one time in the frontal and/or occipital region at an impact velocity of approximately 8.3 meters per second (18.5 mph), which was verified computationally. Repeatability of the tests was confirmed at the start and end of data collection by dropping the Hybrid III headform from a height of 2.0 m onto a Modular Elastomer Programmer (MEP) pad of 25 mm thickness and durometer 60A. Standard Error of the Mean of 0.061 was computed based on peak angular accelerations for pre and post MEP pad drop tests.
Five samples of each motorcycle helmet model were purchased in new condition. Each helmet was impacted one time in the frontal and/or occipital region at an impact velocity of approximately 8.3 meters per second (18.5 mph), which was verified computationally. Repeatability of the tests was confirmed at the start and end of data collection by dropping the Hybrid III headform from a height of 2.0 m onto a Modular Elastomer Programmer (MEP) pad of 25 mm thickness and durometer 60A. Standard Error of the Mean of 0.061 was computed based on peak angular accelerations for pre and post MEP pad drop tests.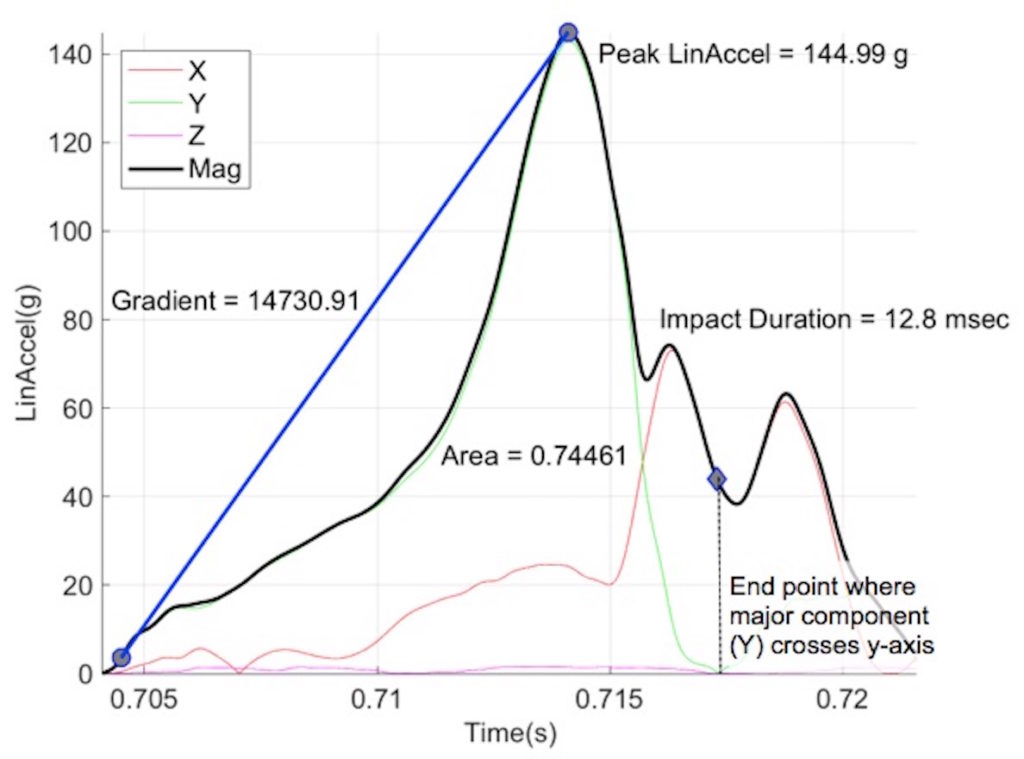 An analysis method validated by Takhounts
An analysis method validated by Takhounts